

The Diagnosis and Treatment of Ectopic Pregnancy
- PMID: 26554319
- PMCID: PMC4643163
- DOI: 10.3238/arztebl.2015.0693
The Diagnosis and Treatment of Ectopic Pregnancy
Abstract
Background: Extrauterine pregnancy is a complication of the first trimester of pregnancy that arises in 1.3-2.4% of all pregnancies.
Methods: This review is based on articles and guidelines retrieved by a selective PubMed search.
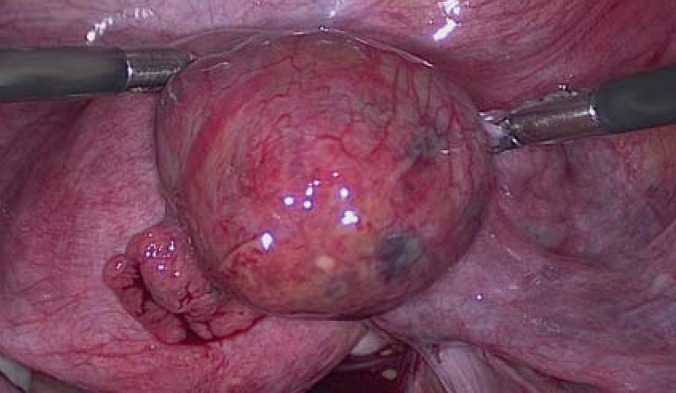
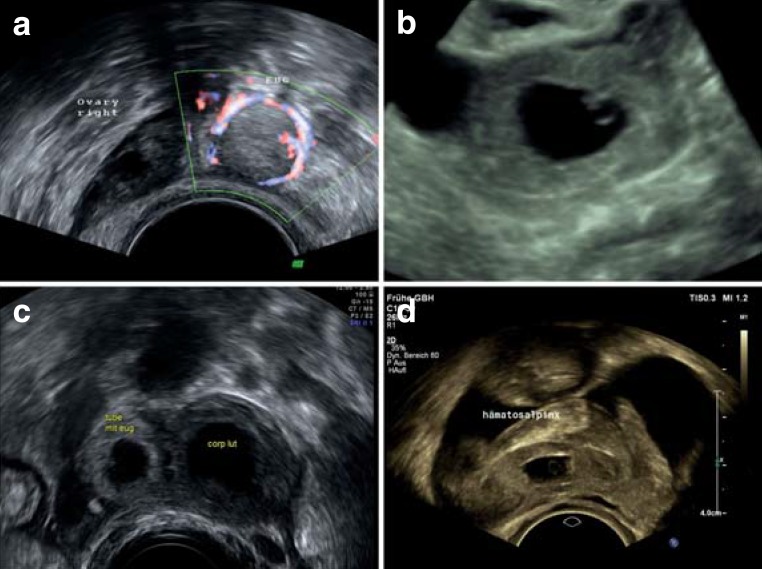
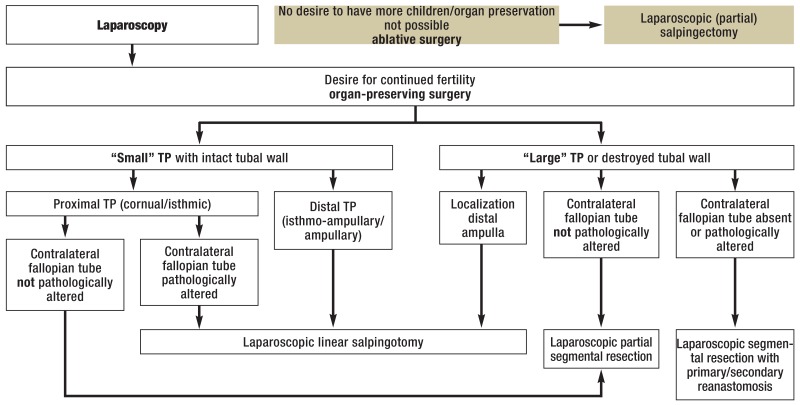
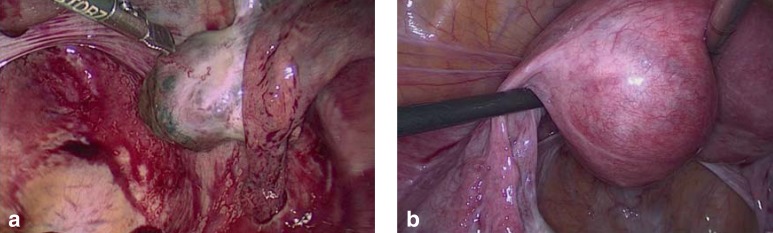
Results: The presentation of extrauterine pregnancy is highly variable, ranging from an asymptomatic state, to pelvic pain that is worse on one side, to tubal rupture with hemorrhagic shock. 75% of tubal pre gnancies can be detected by transvaginal ultrasonography. In patients with a vital extrauterine pregnancy, the human chorionic gonadotropin concentration generally doubles within 48 hours. Laparoscopy is the gold standard of treatment. Two randomized, controlled trials comparing organ-preserving treatment with ablative surgery revealed no significant difference in pregnancy rates after the intervention, but precise details of the surgical procedures were not provided, and long-term fertility data are lacking. Metho - trexate therapy should be used only for strict indications.
Conclusion: Further randomized, controlled trials with longer follow-up will be needed to answer currently open questions about the potential for individualized surgical treatment and the proper role of pharmacotherapy.
Figures
References
-
- Farquhar CM. Ectopic pregnancy. Lancet. 2005;366:583–591. - PubMed
-
- Barnhart KT. Clinical practice. Ectopic pregnancy. N Engl J Med. 2009;361:379–387. - PubMed
-
- Khan KS, Wojdyla D, Say L, Gülmezoglu AM, van Look PF. WHO analysis of causes of maternal death: a systematic review. Lancet. 2006;367:1066–1074. - PubMed
-
- Mikolajczyk RT, Kraut AA, Garbe E. Evaluation of pregnancy outcome records in the German Pharmacoepidemiological Research Database (GePaRD) Pharmacoepidemiol Drug Saf. 2013;22:873–880. - PubMed
-
- Marion LL, Meeks GR. Ectopic pregnancy: History, incidence, epidemiology, and risk factors. Clin Obstet Gynecol. 2012;55:376–386. - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical