

Race- and Sex-Specific Incidence Rates and Predictors of Total Knee Arthroplasty: Seven-Year Data From the Osteoarthritis Initiative
- PMID: 26554629
- PMCID: PMC4862940
- DOI: 10.1002/acr.22771
Race- and Sex-Specific Incidence Rates and Predictors of Total Knee Arthroplasty: Seven-Year Data From the Osteoarthritis Initiative
Abstract
Objective: To determine race- and sex-specific rates of total knee arthroplasty (TKA) and to document independent effects of demographic factors on TKA incidence in a population with radiographically confirmed osteoarthritis (OA).
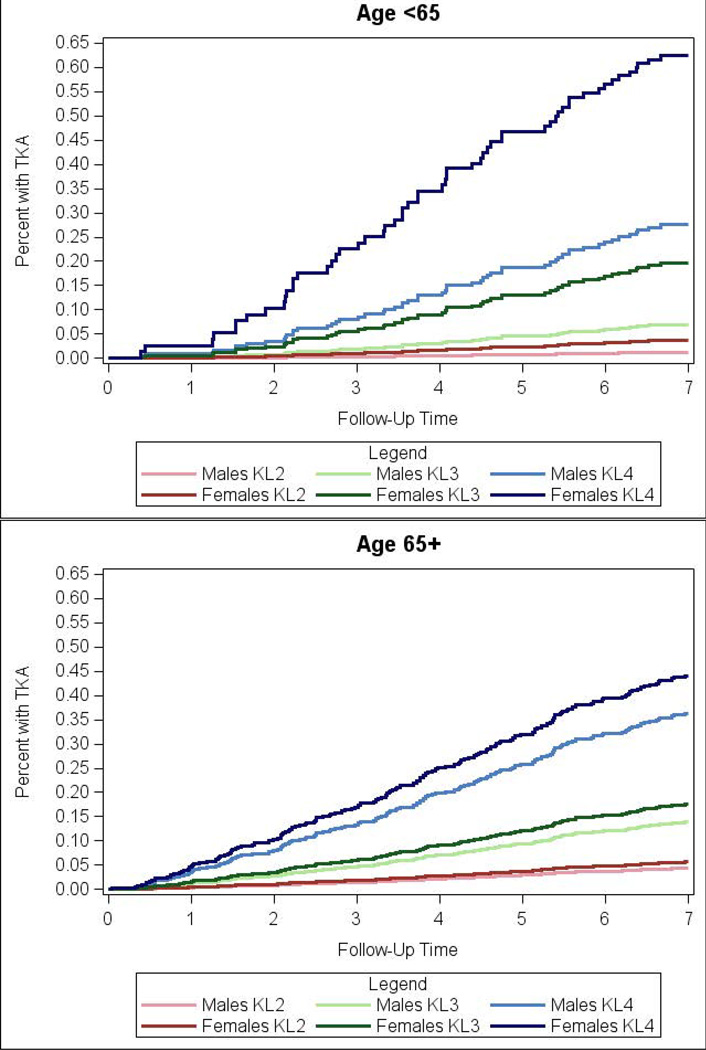
Methods: We used data from the Osteoarthritis Initiative, a US-based, multicenter longitudinal study of knee OA. We selected subjects with radiographic symptomatic OA at baseline and determined TKA incidence rates (ratio of TKAs to time at risk for TKA) over 84 months of followup. We used multivariable Poisson regression to identify independent associations between demographic factors and TKA utilization.
Results: During the study period there were 223 TKAs among 1,915 subjects for an incidence of 1.9% (95% confidence interval [95% CI] 1.7-2.2%). The overall rate was 1.9% (95% CI 1.5-2.3%) in men versus 2.0% (95% CI 1.7-2.3%) in women, and 2.2% (95% CI 1.9-2.6%) in whites versus 1.0% (95% CI 0.7-1.5%) in nonwhites. We observed a statistically significant interaction between sex and age (stratified at <65 and ≥65 years at end of followup), wherein male sex was associated with decreased risk of TKA for younger participants (relative risk [RR] 0.32) but not for older participants. Nonwhite race was associated with a decreased risk of TKA for both younger (RR 0.32) and older (RR 0.43) participants.
Conclusion: Our finding that nonwhites were less likely to undergo TKA than whites in adjusted analyses confirms racial differences observed in population-based studies and underscores the need for interventions to address lower use of TKA among nonwhites with OA.
Trial registration: ClinicalTrials.gov NCT00080171.
© 2016, American College of Rheumatology.
Conflict of interest statement
The authors do not have any conflict of interest with respect to the content of this paper.
Figures

References
-
- Paxton EW, Namba RS, Maletis GB, Khatod M, Yue EJ, Davies M, et al. A prospective study of 80,000 total joint and 5000 anterior cruciate ligament reconstruction procedures in a community-based registry in the United States. J Bone Joint Surg Am. 2010;92(Suppl 2):117–132. - PubMed
-
- Ethgen O, Bruyere O, Richy F, Dardennes C, Reginster JY. Health-related quality of life in total hip and total knee arthroplasty A qualitative and systematic review of the literature. J Bone Joint Surg Am. 2004;86:963–974. - PubMed
Publication types
MeSH terms
Associated data
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
