

Children With Intracranial Arachnoid Cysts: Classification and Treatment
- PMID: 26554773
- PMCID: PMC4915874
- DOI: 10.1097/MD.0000000000001749
Children With Intracranial Arachnoid Cysts: Classification and Treatment
Abstract
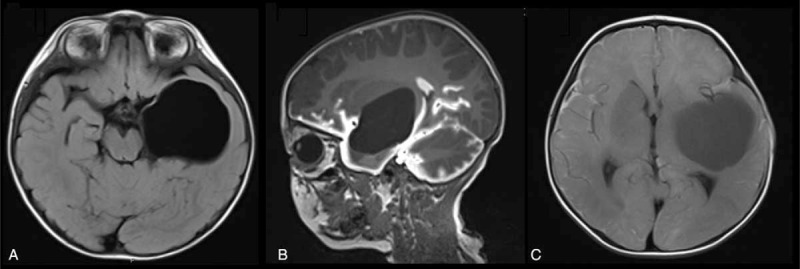
We performed a dynamic study of arachnoid cysts (ACs) using magnetic resonance cisternography (MRC) and proposed a classification of ACs.Twenty-three suitable patients in our hospital entered into this study according to our inclusion criteria. MRC images were collected in all the subjects at 1 and 24 hours after the administration of intrathecal gadolinium-diethylenetriamine penta-acetic acid (Gd-DTPA). We allocate the enrolled patients into 2 groups, MRC group and surgery group. The MRC results were considered before treatment in 1 group (MRC group, 13 patients), whereas another group was surgically treated without considering the MRC results (surgery group, 10 patients). We calculated the enhanced area of cyst using modified MacDonald Criteria from the images and measured the surrounding subarachnoid area as the reference.We found that it was practically useful to quantify 3 types of ACs, complete communicating, incomplete communicating, and noncommunicating, according to MRC results in this study. All the subjects in both groups are closely observed before the treatment and the follow-up using the MRI examination. In the surgery group, 5 patients were found that the area of cysts shrank in the follow-up stage. However, there was no significant difference in the percentage shrinkage area between the 2 groups.We concluded that MRC with Gd-DTPA as a contrast agent is of significant clinical value for the diagnosis and treatment of children with intracranial ACs. This classification based on dynamic MRC is useful for making surgical recommendations.
Conflict of interest statement
The authors have no conflicts of interest to disclose.
Figures



Similar articles
-
CT cisternography in intracranial symptomatic arachnoid cysts: classification and treatment.J Neurol Sci. 2012 Jul 15;318(1-2):125-30. doi: 10.1016/j.jns.2012.03.008. Epub 2012 Apr 19. J Neurol Sci. 2012. PMID: 22520095 Clinical Trial.
-
Phase-contrast cine MRI versus MR cisternography on the evaluation of the communication between intraventricular arachnoid cysts and neighbouring cerebrospinal fluid spaces.Neuroradiology. 2009 May;51(5):305-12. doi: 10.1007/s00234-009-0499-6. Epub 2009 Jan 27. Neuroradiology. 2009. PMID: 19172255
-
Intrathecal gadolinium (gadopentetate dimeglumine)-enhanced MR cisternography used to determine potential communication between the cerebrospinal fluid pathways and intracranial arachnoid cysts.Neuroradiology. 2004 Sep;46(9):744-54. doi: 10.1007/s00234-004-1240-0. Neuroradiology. 2004. PMID: 15289956 Clinical Trial.
-
Neuroendoscopic management of suprasellar arachnoid cysts.World Neurosurg. 2013 Feb;79(2 Suppl):S19.e13-8. doi: 10.1016/j.wneu.2012.02.011. Epub 2012 Feb 10. World Neurosurg. 2013. PMID: 22381821 Review.
-
Intradural Spinal Arachnoid Cyst: A Long-Term Postlaminectomy Complication: A Case Report and Review of the Literature.World Neurosurg. 2016 Jan;85:367.e1-4. doi: 10.1016/j.wneu.2015.09.058. Epub 2015 Sep 30. World Neurosurg. 2016. PMID: 26428320 Review.
Cited by
-
Acetazolamide to treat symptomatic ruptured arachnoid cysts: illustrative cases.J Neurosurg Case Lessons. 2022 Apr 18;3(16):CASE21462. doi: 10.3171/CASE21462. Print 2022 Apr 18. J Neurosurg Case Lessons. 2022. PMID: 36303495 Free PMC article.
-
Familial and syndromic forms of arachnoid cyst implicate genetic factors in disease pathogenesis.Cereb Cortex. 2023 Mar 10;33(6):3012-3025. doi: 10.1093/cercor/bhac257. Cereb Cortex. 2023. PMID: 35851401 Free PMC article.
-
Ophthalmological symptoms in children with intracranial cysts.Sci Rep. 2017 Oct 19;7(1):13630. doi: 10.1038/s41598-017-13266-7. Sci Rep. 2017. PMID: 29051539 Free PMC article.
-
Expanding the genetic spectrum of giant axonal neuropathy: Two novel variants in Iranian families.Mol Genet Genomic Med. 2023 Jun;11(6):e2159. doi: 10.1002/mgg3.2159. Epub 2023 Mar 3. Mol Genet Genomic Med. 2023. PMID: 36866531 Free PMC article. Review.
-
Progressive Quadriparesis of a Toddler with a Posterior Cranial Fossa Arachnoid Cyst (AC): Illustrative Case Report and Narrative Literature Review.Children (Basel). 2024 Nov 29;11(12):1463. doi: 10.3390/children11121463. Children (Basel). 2024. PMID: 39767892 Free PMC article.
References
-
- Lorenz M, Niedermaier N, Lowitzsch K. Arachnoid cyst and tension headache: symptom or accidental finding? Schmerz (Berlin, Germany) 2002; 16:304–307. - PubMed
-
- Wester K. Peculiarities of intracranial arachnoid cysts: location, sidedness, and sex distribution in 126 consecutive patients. Neurosurgery 1999; 45:775. - PubMed
-
- Cincu R, Agrawal A, Eiras J. Intracranial arachnoid cysts: current concepts and treatment alternatives. Clin Neurol Neurosurg 2007; 109:837–843. - PubMed
-
- Choi JW, Lee JY, Phi JH, et al. Stricter indications are recommended for fenestration surgery in intracranial arachnoid cysts of children. Child's Nervous System 2014; 31:77–86. - PubMed
-
- Kandenwein J, Richter H-P, Börm W. Surgical therapy of symptomatic arachnoid cysts—an outcome analysis. Acta Neurochir 2004; 146:1317–1322. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
