

Meta-Analysis and Cost Comparison of Empirical versus Pre-Emptive Antifungal Strategies in Hematologic Malignancy Patients with High-Risk Febrile Neutropenia
- PMID: 26554923
- PMCID: PMC4640557
- DOI: 10.1371/journal.pone.0140930
Meta-Analysis and Cost Comparison of Empirical versus Pre-Emptive Antifungal Strategies in Hematologic Malignancy Patients with High-Risk Febrile Neutropenia
Abstract
Background: Invasive fungal disease (IFD) causes significant morbidity and mortality in hematologic malignancy patients with high-risk febrile neutropenia (FN). These patients therefore often receive empirical antifungal therapy. Diagnostic test-guided pre-emptive antifungal therapy has been evaluated as an alternative treatment strategy in these patients.
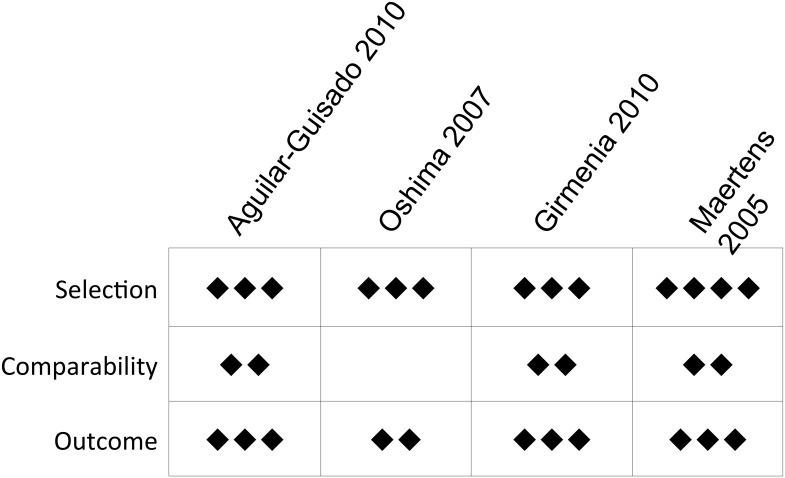
Methods: We conducted an electronic search for literature comparing empirical versus pre-emptive antifungal strategies in FN among adult hematologic malignancy patients. We systematically reviewed 9 studies, including randomized-controlled trials, cohort studies, and feasibility studies. Random and fixed-effect models were used to generate pooled relative risk estimates of IFD detection, IFD-related mortality, overall mortality, and rates and duration of antifungal therapy. Heterogeneity was measured via Cochran's Q test, I2 statistic, and between study τ2. Incorporating these parameters and direct costs of drugs and diagnostic testing, we constructed a comparative costing model for the two strategies. We conducted probabilistic sensitivity analysis on pooled estimates and one-way sensitivity analyses on other key parameters with uncertain estimates.
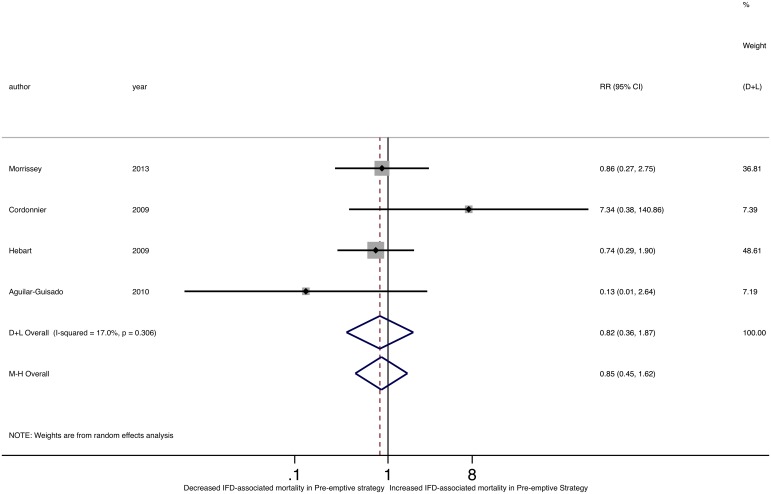
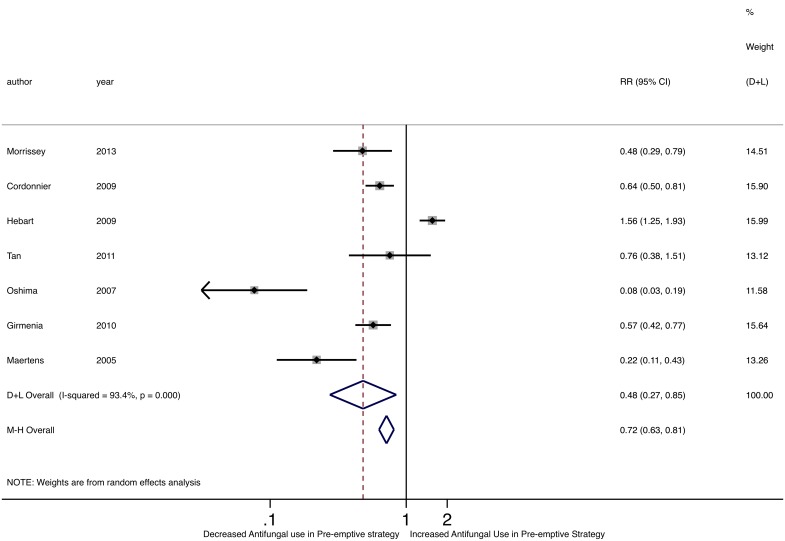
Results: Nine published studies met inclusion criteria. Compared to empirical antifungal therapy, pre-emptive strategies were associated with significantly lower antifungal exposure (RR 0.48, 95% CI 0.27-0.85) and duration without an increase in IFD-related mortality (RR 0.82, 95% CI 0.36-1.87) or overall mortality (RR 0.95, 95% CI 0.46-1.99). The pre-emptive strategy cost $324 less (95% credible interval -$291.88 to $418.65 pre-emptive compared to empirical) than the empirical approach per FN episode. However, the cost difference was influenced by relatively small changes in costs of antifungal therapy and diagnostic testing.
Conclusions: Compared to empirical antifungal therapy, pre-emptive antifungal therapy in patients with high-risk FN may decrease antifungal use without increasing mortality. We demonstrate a state of economic equipoise between empirical and diagnostic-directed pre-emptive antifungal treatment strategies, influenced by small changes in cost of antifungal therapy and diagnostic testing, in the current literature. This work emphasizes the need for optimization of existing fungal diagnostic strategies, development of more efficient diagnostic strategies, and less toxic and more cost-effective antifungals.
Conflict of interest statement
Figures





Similar articles
-
Pre-emptive diagnosis and treatment of fungal infections--evaluation of a single-centre policy.Clin Microbiol Infect. 2012 Feb;18(2):189-94. doi: 10.1111/j.1469-0691.2011.03589.x. Epub 2011 Jul 6. Clin Microbiol Infect. 2012. PMID: 21729194
-
A hematology consensus agreement on antifungal strategies for neutropenic patients with hematological malignancies and stem cell transplant recipients. Gruppo Italiano Malattie Ematologiche dell'Adulto, Gruppo Italiano Trapianto di Midollo Osseo, Associazione Italiana Ematologia ed Oncologia Pediatrica, Invasive Fungal Infections Cooperative Group of the European Organization for Research and Treatment of Cancer and Sorveglianza Epidemiologica delle Infezioni Fungine nelle Emopatie Maligne.Hematol Oncol. 2013 Sep;31(3):117-26. doi: 10.1002/hon.2031. Epub 2012 Oct 5. Hematol Oncol. 2013. PMID: 23037867
-
Empirical versus preemptive antifungal therapy for high-risk, febrile, neutropenic patients: a randomized, controlled trial.Clin Infect Dis. 2009 Apr 15;48(8):1042-51. doi: 10.1086/597395. Clin Infect Dis. 2009. PMID: 19281327 Clinical Trial.
-
A cost and resource utilization analysis of micafungin bridging for hemato-oncological high-risk patients undergoing allogeneic stem cell transplantation.Eur J Haematol. 2015 Jun;94(6):526-31. doi: 10.1111/ejh.12466. Epub 2015 Feb 23. Eur J Haematol. 2015. PMID: 25310918
-
Antifungal pre-emptive strategy for high-risk neutropenic patients: why the story is still ongoing.Clin Microbiol Infect. 2014 Jun;20 Suppl 6:27-35. doi: 10.1111/1469-0691.12428. Epub 2014 Jan 28. Clin Microbiol Infect. 2014. PMID: 24283975 Review.
Cited by
-
Comparing Invasive Pulmonary Aspergillosis Mortality Between Liposomal Amphotericin B and Voriconazole in Patients With Hematological Malignancy or Hematopoietic Stem Cell Transplantation.Cureus. 2022 Nov 21;14(11):e31762. doi: 10.7759/cureus.31762. eCollection 2022 Nov. Cureus. 2022. PMID: 36569688 Free PMC article.
-
Tackling the emerging threat of antifungal resistance to human health.Nat Rev Microbiol. 2022 Sep;20(9):557-571. doi: 10.1038/s41579-022-00720-1. Epub 2022 Mar 29. Nat Rev Microbiol. 2022. PMID: 35352028 Free PMC article. Review.
-
Adherence to, and outcomes of, a galactomannan screening protocol in high-risk hematology patients.Curr Oncol. 2018 Apr;25(2):e139-e145. doi: 10.3747/co.25.3848. Epub 2018 Apr 30. Curr Oncol. 2018. PMID: 29719438 Free PMC article.
-
Treatment Effects in Randomized and Nonrandomized Studies of Pharmacological Interventions: A Meta-Analysis.JAMA Netw Open. 2024 Sep 3;7(9):e2436230. doi: 10.1001/jamanetworkopen.2024.36230. JAMA Netw Open. 2024. PMID: 39331390 Free PMC article.
-
Challenges in the Treatment of Invasive Aspergillosis in Immunocompromised Children.Antimicrob Agents Chemother. 2022 Jul 19;66(7):e0215621. doi: 10.1128/aac.02156-21. Epub 2022 Jun 29. Antimicrob Agents Chemother. 2022. PMID: 35766509 Free PMC article. Review.
References
-
- Vartivarian SE, Anaissie EJ, Bodey GP. Emerging fungal pathogens in immunocompromised patinets: classification, diagnosis, and management. Clin Infect Dis, 1993; 17: Suppl 2: S487–489. - PubMed
-
- Kontoyiannis DP, Marr KA, Park BJ, Alexander BD, Anaissie EJ, Walsh TJ, et al. Prospective surveillance for invasive fungal infections in hematopoietic stem cell transplant recipients, 2001–2006: overview of the Transplant-Associated Infection Surveillance Network (TRANSNET) Database. Clin Infect Dis, 2010; 50: 1091–1100. 10.1086/651263 - DOI - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Miscellaneous
