

Post-hoc analysis of vitamin D status and reduced risk of preterm birth in two vitamin D pregnancy cohorts compared with South Carolina March of Dimes 2009-2011 rates
- PMID: 26554936
- PMCID: PMC5215876
- DOI: 10.1016/j.jsbmb.2015.10.022
Post-hoc analysis of vitamin D status and reduced risk of preterm birth in two vitamin D pregnancy cohorts compared with South Carolina March of Dimes 2009-2011 rates
Abstract
Background: Two vitamin D pregnancy supplementation trials were recently undertaken in South Carolina: The NICHD (n=346) and Thrasher Research Fund (TRF, n=163) studies. The findings suggest increased dosages of supplemental vitamin D were associated with improved health outcomes of both mother and newborn, including risk of preterm birth (<37 weeks gestation). How that risk was associated with 25(OH)D serum concentration, a better indicator of vitamin D status than dosage, by race/ethnic group and the potential impact in the community was not previously explored. While a recent IOM report suggested a concentration of 20 ng/mL should be targeted, more recent work suggests optimal conversion of 25(OH)D-1,25(OH)2D takes place at 40 ng/mL in pregnant women.
Objective: Post-hoc analysis of the relationship between 25(OH)D concentration and preterm birth rates in the NICHD and TRF studies with comparison to Charleston County, South Carolina March of Dimes (CC-MOD) published rates of preterm birth to assess potential risk reduction in the community.
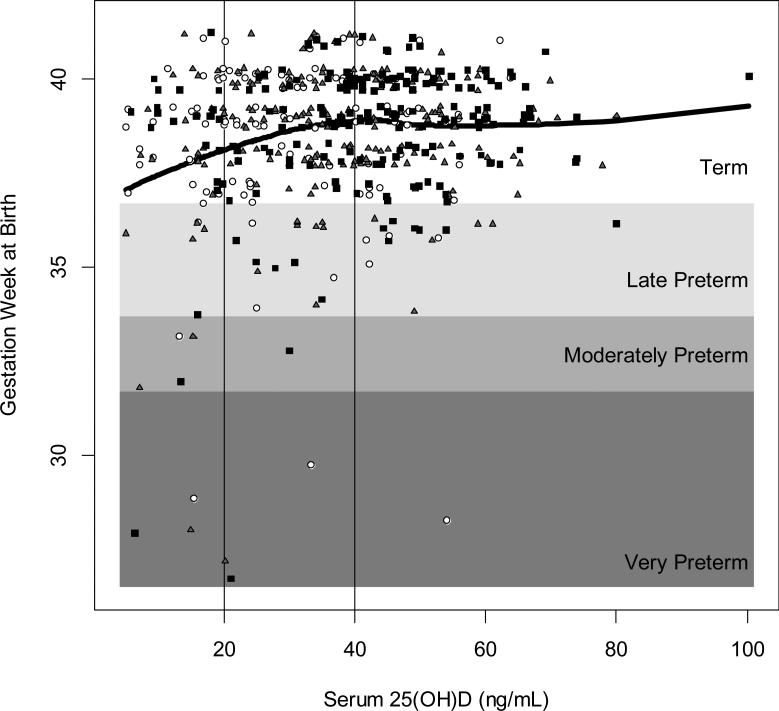
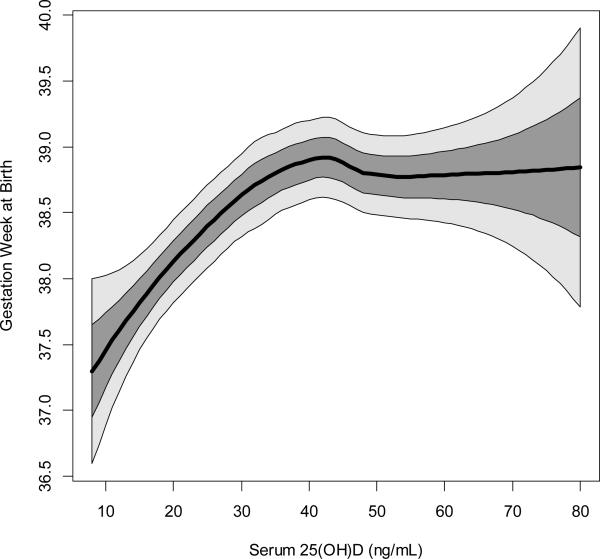
Methods: Using the combined cohort datasets (n=509), preterm birth rates both for the overall population and for the subpopulations achieving 25(OH)D concentrations of ≤20 ng/mL, >20 to <40 ng/mL, and ≥40 ng/mL were calculated; subpopulations broken down by race/ethnicity were also examined. Log-binomial regression was used to test if an association between 25(OH)D serum concentration and preterm birth was present when adjusted for covariates; locally weighted regression (LOESS) was used to explore the relationship between 25(OH)D concentration and gestational age (weeks) at delivery in more detail. These rates were compared with 2009-2011 CC-MOD data to assess potential risk reductions in preterm birth.
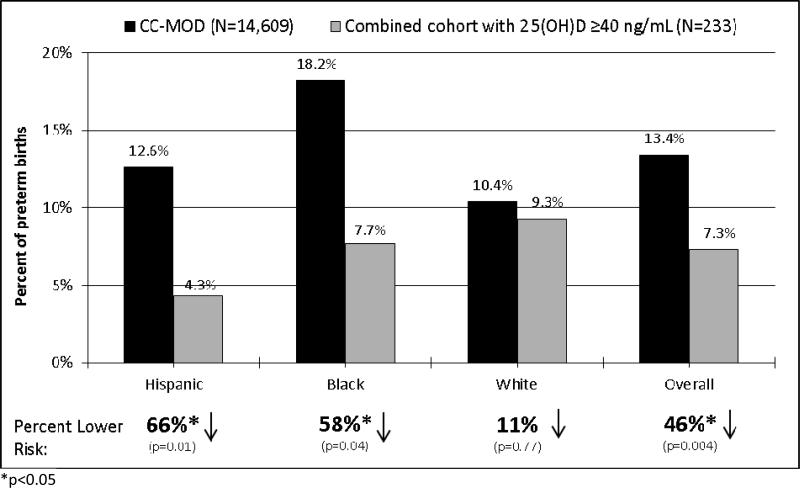
Results: Women with serum 25(OH)D concentrations ≥40 ng/mL (n=233) had a 57% lower risk of preterm birth compared to those with concentrations ≤20 ng/mL [n=82; RR=0.43, 95% confidence interval (CI)=0.22,0.83]; this lower risk was essentially unchanged after adjusting for covariates (RR=0.41, 95% CI=0.20,0.86). The fitted LOESS curve shows gestation week at birth initially rising steadily with increasing 25(OH)D and then plateauing at ∼40 ng/mL. Broken down by race/ethnicity, there was a 79% lower risk of preterm birth among Hispanic women with 25(OH)D concentrations ≥40 ng/mL (n=92) compared to those with 25(OH)D concentrations ≤20 ng/mL (n=29; RR=0.21, 95% CI=0.06,0.69) and a 45% lower risk among Black women (n=52 and n=50; RR=0.55, 95% CI=0.17,1.76). There were too few white women with low 25(OH)D concentrations for assessment (n=3). Differences by race/ethnicity were not statistically significant with 25(OH)D included as a covariate. Compared to the CC-MOD reference group, women with serum concentrations ≥40 ng/mL in the combined cohort had a 46% lower rate of preterm birth overall (n=233, p=0.004) with a 66% lower rate among Hispanic women (n=92, p=0.01) and a 58% lower rate among black women (n=52, p=0.04).
Conclusions: In this post-hoc analysis, achieving a 25(OH)D serum concentration ≥40 ng/mL significantly decreased the risk of preterm birth compared to ≤20 ng/mL. These findings suggest the importance of raising 25(OH)D levels substantially above 20 ng/mL; reaching 40 ng/mL during pregnancy would reduce the risk of preterm birth and achieve the maximal production of the active hormone.
Keywords: Cholecalciferol; March of Dimes; Pregnancy health outcomes; Preterm birth; Vitamin D.
Copyright © 2015 The Authors. Published by Elsevier Ltd.. All rights reserved.
Figures
References
-
- Holick MF. Vitamin D Deficiency. 2007;357(3):266–81. doi: 10.1056/NEJMra070553. - PubMed
-
- Bikle DD. Vitamin D and the immune system: role in protection against bacterial infection. Curr Opin Nephrol Hypertens. 2008;17(4):348–52. Epub 2008/07/29. doi: 10.1097/MNH.0b013e3282ff64a3 00041552-200807000-00003 [pii]. PubMed PMID: 18660668. - PubMed
-
- Liu P, Stenger S, Tang D, Modlin R. Cutting edge: vitamin D-mediated human antimicrobial activity against Mycobacterium tuberculosis is dependent on the induction of cathelicidin. J Immunol. 2007;179:2060–3. - PubMed
-
- Wagner CL, Baggerly C, McDonnell SL, Baggerly L, Hamilton SA, Winkler J, Warner G, Rodriguez C, Shary JR, Smith PG, Hollis BW. Post-hoc comparison of vitamin D status at three timepoints during pregnancy demonstrates lower risk of preterm birth with higher vitamin D closer to delivery. The Journal of steroid biochemistry and molecular biology. 2014 doi: 10.1016/j.jsbmb.2014.11.013. PubMed PMID: 25448734. - PMC - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
