

Health and Economic Implications of National Treatment Coverage for Cardiovascular Disease in India: Cost-Effectiveness Analysis
- PMID: 26555122
- PMCID: PMC4801228
- DOI: 10.1161/CIRCOUTCOMES.115.001994
Health and Economic Implications of National Treatment Coverage for Cardiovascular Disease in India: Cost-Effectiveness Analysis
Abstract
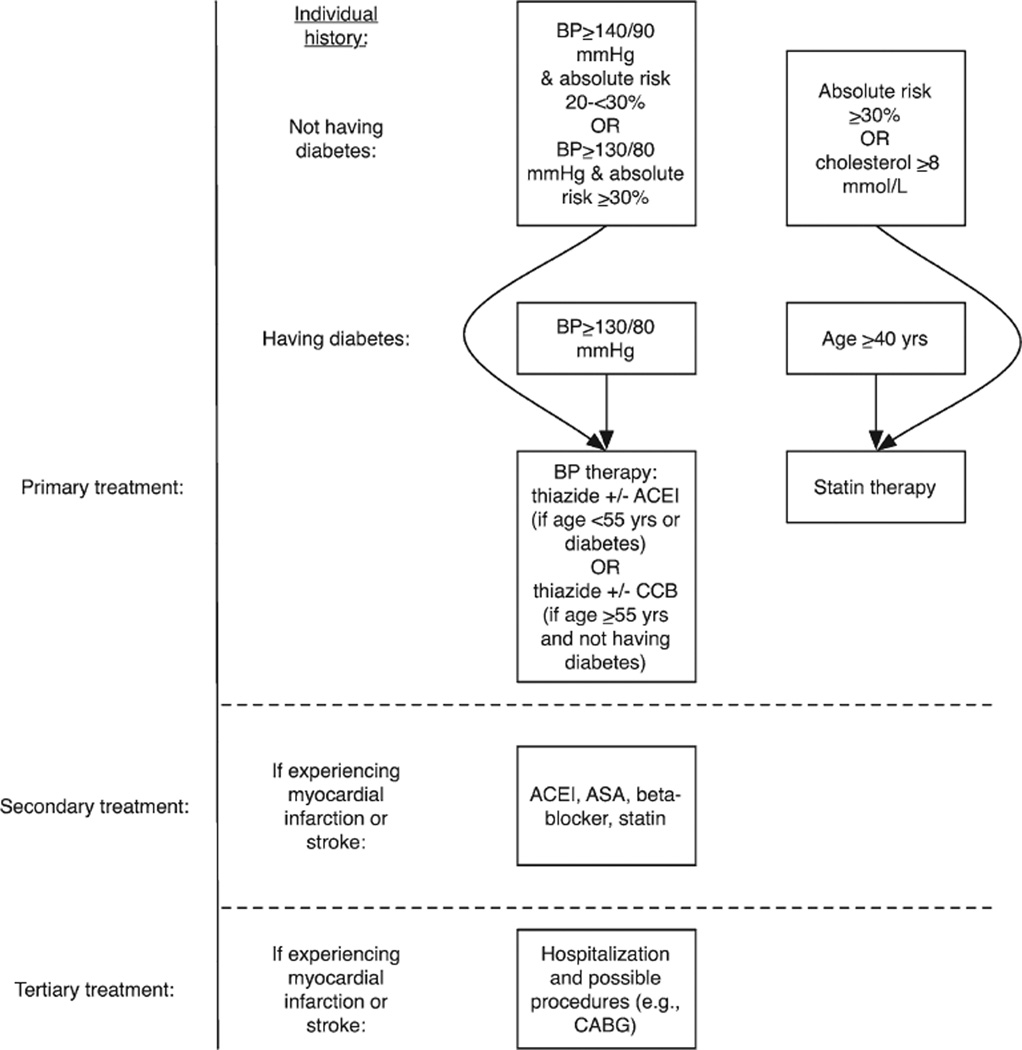
Background: Whether to cover cardiovascular disease costs is an increasingly pressing question for low- and middle-income countries. We sought to identify the impact of expanding national insurance to cover primary prevention, secondary prevention, and tertiary treatment for cardiovascular disease in India.
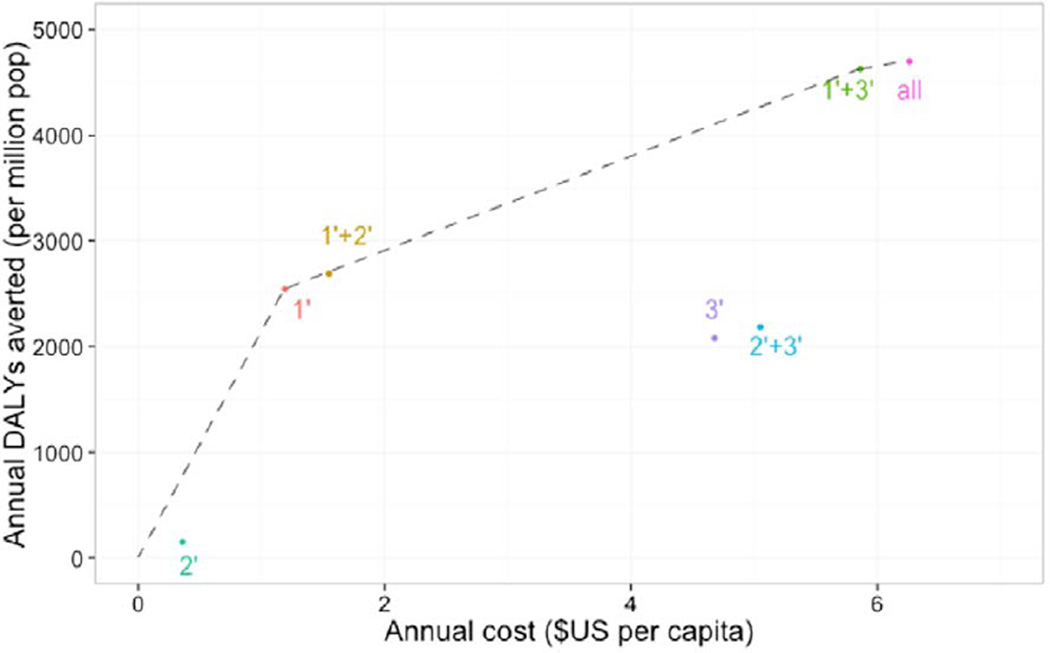
Methods and results: We incorporated data from coverage experiments into a validated microsimulation model of myocardial infarction and stroke in India to evaluate the cost-effectiveness of alternate coverage strategies. Coverage of primary prevention alone saved 3.6 million disability-adjusted life-years (DALY) per annum at an incremental cost-effectiveness ratio of $469 per DALY averted when compared with the status quo of no coverage. Coverage of primary and secondary preventions was dominated by a strategy of covering primary prevention and tertiary treatment, which prevented 6.6 million DALYs at an incremental cost-effectiveness ratio of $2241 per DALY averted, when compared with that of primary prevention alone. The combination of all 3 categories yielded the greatest impact at an incremental cost per DALY averted of $5588 when compared with coverage of primary prevention plus tertiary treatment. When compared with the status quo of no coverage, coverage of all 3 categories of prevention/treatment yielded an incremental cost-effectiveness ratio of $1331 per DALY averted. In sensitivity analyses, coverage of primary preventive treatments remained cost-effective even if adherence and access to therapy were low, but tertiary coverage would require avoiding unnecessary procedures to remain cost-effective.
Conclusions: Coverage of all 3 major types of cardiovascular treatment would be expected to have high impact and reasonable cost-effectiveness in India across a broad spectrum of access and adherence levels.
Keywords: cost-effectiveness; developing countries; health policy; healthcare economics and organizations; insurance; myocardial infarction; stroke.
© 2015 American Heart Association, Inc.
Figures
Comment in
-
The Devil Is in the Details: Achieving Reductions in Global Cardiovascular Disease Mortality.Circ Cardiovasc Qual Outcomes. 2015 Nov;8(6):535-8. doi: 10.1161/CIRCOUTCOMES.115.002314. Epub 2015 Nov 10. Circ Cardiovasc Qual Outcomes. 2015. PMID: 26555121 Free PMC article. No abstract available.
References
-
- Alwan A. World Health Organization; 2011. [Accessed July 31, 2015]. Global status report on noncommunicable diseases 2010. [Internet] [cited 2015 Jan 28]. http://www.cabdirect.org/abstracts/20113168808.html.
-
- McKee M, Balabanova D, Basu S, Ricciardi W, Stuckler D. Universal health coverage: a quest for all countries but under threat in some. Value Health. 2013;16(1 suppl):S39–S45. - PubMed
-
- Lim SS, Gaziano TA, Gakidou E, Reddy KS, Farzadfar F, Lozano R, Rodgers A. Prevention of cardiovascular disease in high-risk individuals in low-income and middle-income countries: health effects and costs. Lancet. 2007;370:2054–2062. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
