

Model-Based Optimisation of Deferoxamine Chelation Therapy
- PMID: 26555666
- PMCID: PMC4709373
- DOI: 10.1007/s11095-015-1805-0
Model-Based Optimisation of Deferoxamine Chelation Therapy
Abstract
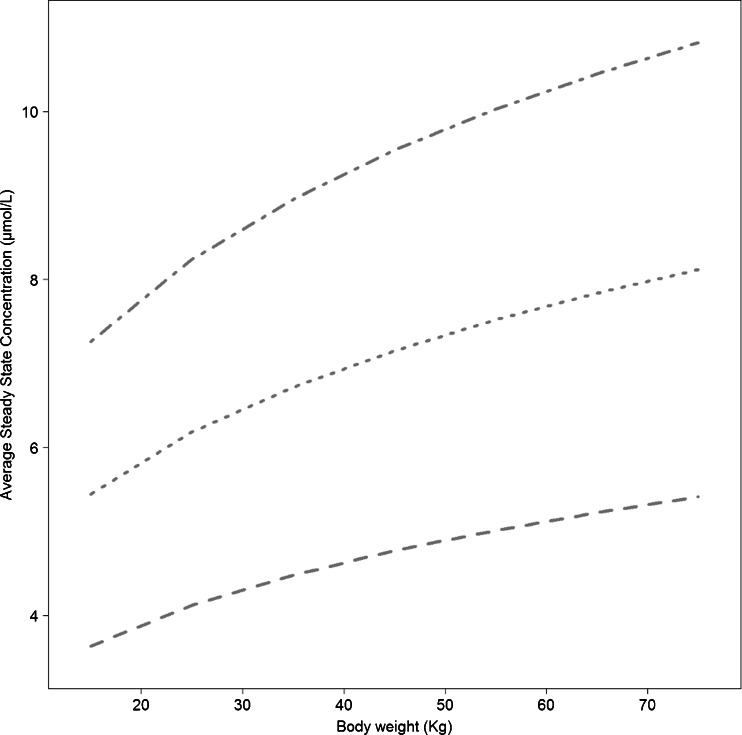
Purpose: Here we show how a model-based approach may be used to provide further insight into the role of clinical and demographic covariates on the progression of iron overload. The therapeutic effect of deferoxamine is used to illustrate the application of disease modelling as a means to characterising treatment response in individual patients.
Methods: Serum ferritin, demographic characteristics and individual treatment data from clinical routine practice on 27 patients affected by β-thalassaemia major were used for the purposes of this analysis. The time course of serum ferritin was described by a hierarchical nonlinear mixed effects model, in which compliance was parameterised as a covariate factor. Modelling and simulation procedures were implemented in NONMEM (7.2.0).
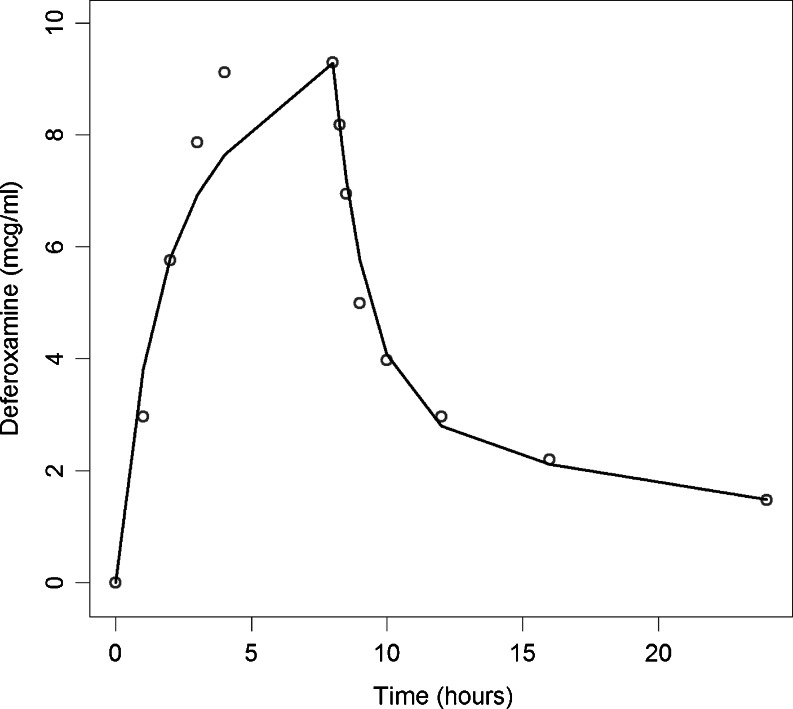
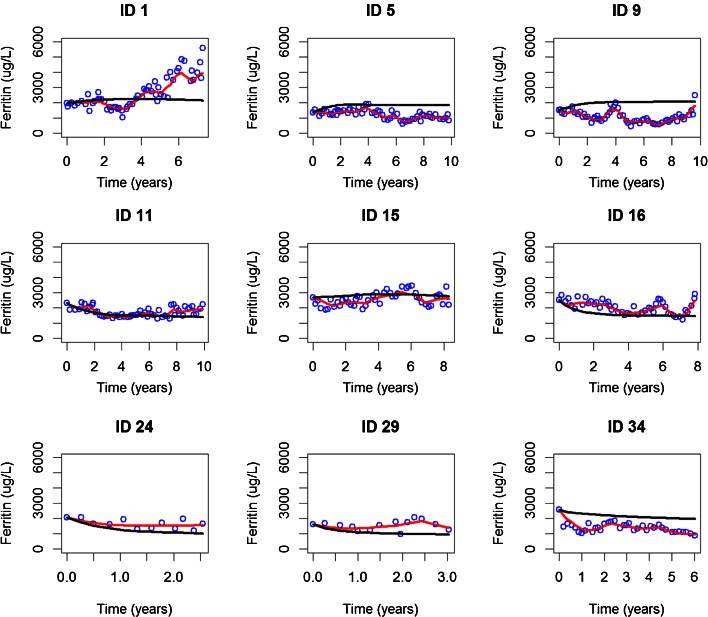
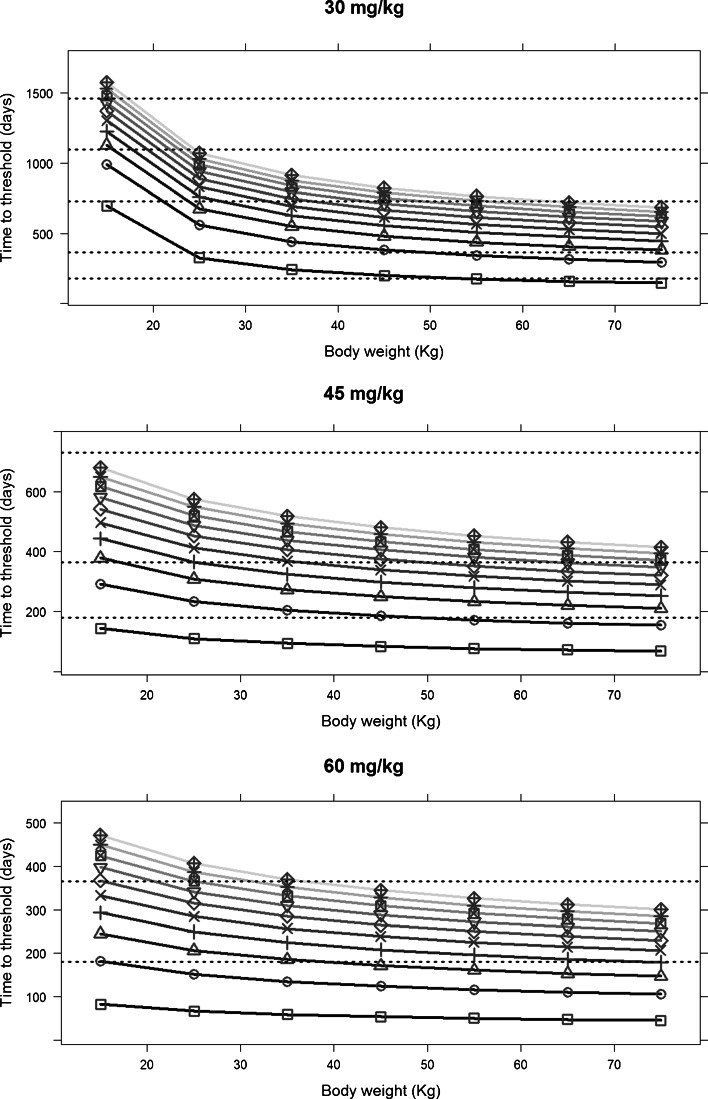
Results: A turnover model best described serum ferritin changes over time, with the effect of blood transfusions introduced on the ferritin conversion rate and the effect of deferoxamine on the elimination parameter (Kout) in a proportional manner. The results of the simulations showed that poor quality of execution is preferable over drug holidays; and that independently of the compliance pattern, the therapeutic intervention is not effective if >60% of the doses are missed.
Conclusions: Modelling of ferritin response enables characterisation of the dynamics of iron overload due to chronic transfusion. The approach can be used to support decision making in clinical practice, including personalisation of the dose for existing and novel chelating agents.
Keywords: PKPD modelling; adherence; deferoxamine; disease modelling; dose rationale; iron overload.
Figures


References
-
- Gibbons R, Higgs DR, Old JM, Olivieri NF, Swee Lay T, Wood WG. The thalassaemia syndromes. 4th edn. Blackwell Sci; 2001.
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
