

Nutritional Modulation of Non-Alcoholic Fatty Liver Disease and Insulin Resistance
- PMID: 26556368
- PMCID: PMC4663582
- DOI: 10.3390/nu7115454
Nutritional Modulation of Non-Alcoholic Fatty Liver Disease and Insulin Resistance
Abstract
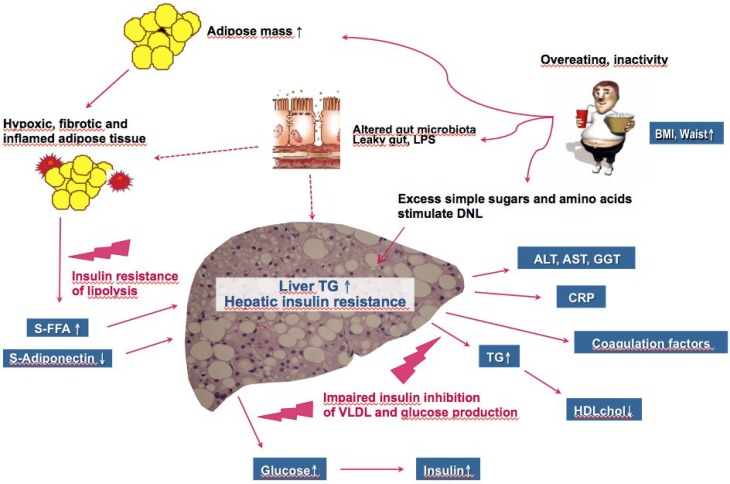
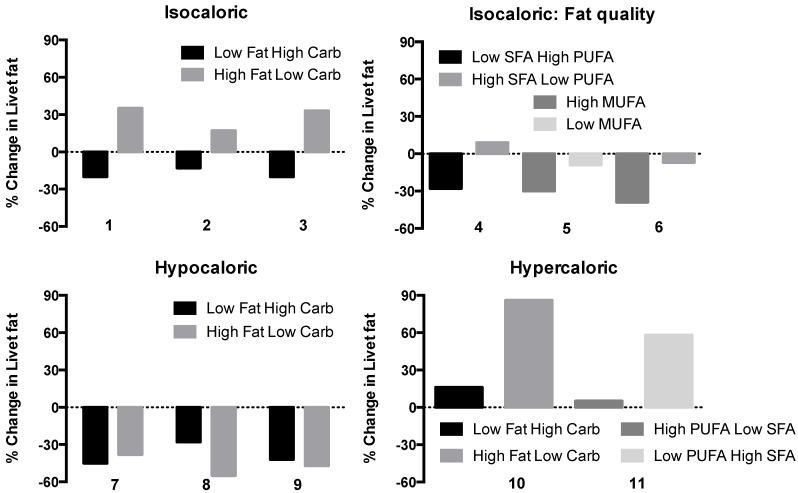
Non-alcoholic fatty liver disease (NAFLD) covers a spectrum of disorders ranging from simple steatosis (non-alcoholic fatty liver, NAFL) to non-alcoholic steatohepatitis (NASH) and cirrhosis. NAFL increases the risk of liver fibrosis. If the liver is fatty due to causes of insulin resistance such as obesity and physical inactivity, it overproduces glucose and triglycerides leading to hyperinsulinemia and a low high-density lipoprotein (HDL) cholesterol concentration. The latter features predispose to type 2 diabetes and cardiovascular disease (CVD). Understanding the impact of nutritional modulation of liver fat content and insulin resistance is therefore of interest for prevention and treatment of NAFLD. Hypocaloric, especially low carbohydrate ketogenic diets rapidly decrease liver fat content and associated metabolic abnormalities. However, any type of caloric restriction seems effective long-term. Isocaloric diets containing 16%-23% fat and 57%-65% carbohydrate lower liver fat compared to diets with 43%-55% fat and 27%-38% carbohydrate. Diets rich in saturated (SFA) as compared to monounsaturated (MUFA) or polyunsaturated (PUFA) fatty acids appear particularly harmful as they increase both liver fat and insulin resistance. Overfeeding either saturated fat or carbohydrate increases liver fat content. Vitamin E supplementation decreases liver fat content as well as fibrosis but has no effect on features of insulin resistance.
Keywords: carbohydrate; fructose; liver fat; saturated fat; steatosis..
Figures
References
-
- Chalasani N., Younossi Z., Lavine J.E., Diehl A.M., Brunt E.M., Cusi K., Charlton M., Sanyal A.J. The diagnosis and management of non-alcoholic fatty liver disease: Practice guideline by the American Gastroenterological Association, American Association for the Study of Liver Diseases, and American College of Gastroenterology. Gastroenterology. 2012;142:1592–1609. doi: 10.1053/j.gastro.2012.04.001. - DOI - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
