

Prospective study of a proactive palliative care rounding intervention in a medical ICU
- PMID: 26556622
- PMCID: PMC4945103
- DOI: 10.1007/s00134-015-4098-1
Prospective study of a proactive palliative care rounding intervention in a medical ICU
Abstract
Purpose: To evaluate the effects of a palliative care intervention on clinical and family outcomes, and palliative care processes.
Methods: Prospective, before-and-after interventional study enrolling patients with high risk of mortality, morbidity, or unmet palliative care needs in a 24-bed academic intensive care unit (ICU). The intervention involved a palliative care clinician interacting with the ICU physicians on daily rounds for high-risk patients.
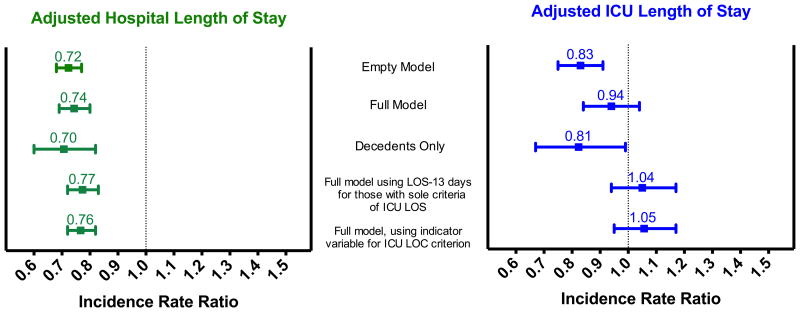
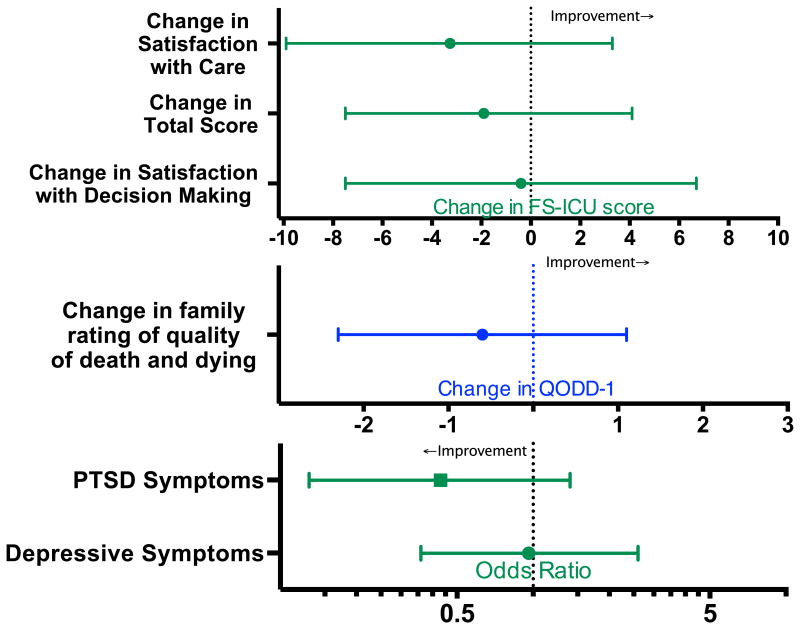
Results: One hundred patients were enrolled in the usual care phase, and 103 patients were enrolled during the intervention phase. The adjusted likelihood of a family meeting in ICU was 63% higher (RR 1.63, 95% CI 1.14-2.07, p = 0.01), and time to family meeting was 41% shorter (95% CI 52-28% shorter, p < 0.001). Adjusted ICU length of stay (LOS) was not significantly different between the two groups (6% shorter, 95% CI 16% shorter to 4% longer, p = 0.22). Among those who died in the hospital, ICU LOS was 19% shorter in the intervention (95% CI 33-1% shorter, p = 0.043). Adjusted hospital LOS was 26% shorter (95% CI 31-20% shorter, p < 0.001) with the intervention. Post-traumatic stress disorder (PTSD) symptoms were present in 9.1% of family respondents during the intervention versus 20.7% prior to the intervention (p = 0.09). Mortality, family depressive symptoms, family satisfaction and quality of death and dying did not significantly differ between groups.
Conclusions: Proactive palliative care involvement on ICU rounds for high-risk patients was associated with more and earlier ICU family meetings and shorter hospital LOS. We did not identify differences in family satisfaction, family psychological symptoms, or family-rated quality of dying, but had limited power to detect such differences.
Keywords: Communication; End-of-life care; Family ICU syndrome; Family meetings; ICU decision-making; Palliative care.
Conflict of interest statement
Figures
Comment in
-
Tasking the tailor to cut the coat: How to optimize individualized ICU-based palliative care?Intensive Care Med. 2016 Jan;42(1):119-21. doi: 10.1007/s00134-015-4107-4. Epub 2015 Nov 10. Intensive Care Med. 2016. PMID: 26556621 No abstract available.
References
-
- Angus DC, Barnato AE, Linde-Zwirble WT, Weissfeld LA, Watson RS, Rickert T, Rubenfeld GD Robert Wood Johnson Foundation ICUE-O-LPG. Use of intensive care at the end of life in the United States: an epidemiologic study. Crit Care Med. 2004;32:638–643. - PubMed
-
- Cox CE, Carson SS, Lindquist JH, Olsen MK, Govert JA, Chelluri L Quality of Life After Mechanical Ventilation in the Aged I. Differences in one-year health outcomes and resource utilization by definition of prolonged mechanical ventilation: a prospective cohort study. Crit Care. 2007;11:R9. - PMC - PubMed
-
- Wunsch H, Guerra C, Barnato AE, Angus DC, Li G, Linde-Zwirble WT. Three-year outcomes for Medicare beneficiaries who survive intensive care. JAMA. 2010;303:849–856. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
