

Gestational Trophoblastic Disorders: An Update in 2015
- PMID: 26556906
- PMCID: PMC4629994
- DOI: 10.1055/s-0035-1558054
Gestational Trophoblastic Disorders: An Update in 2015
Abstract
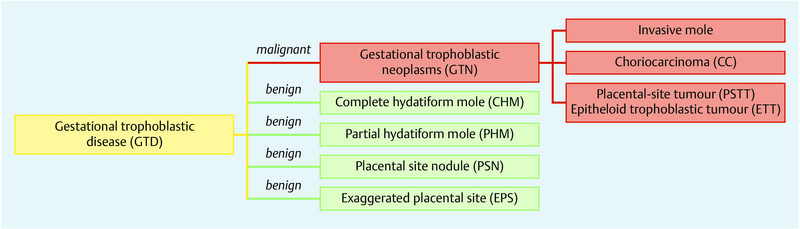
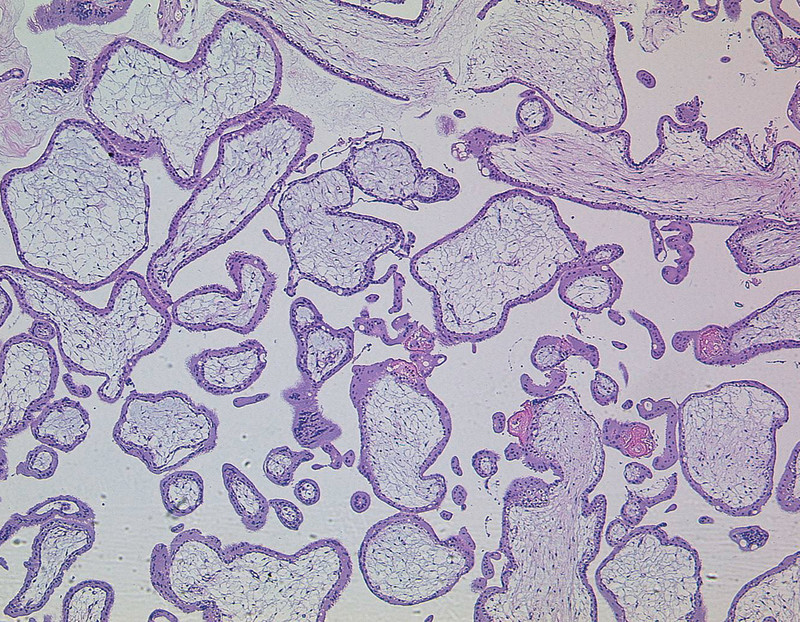
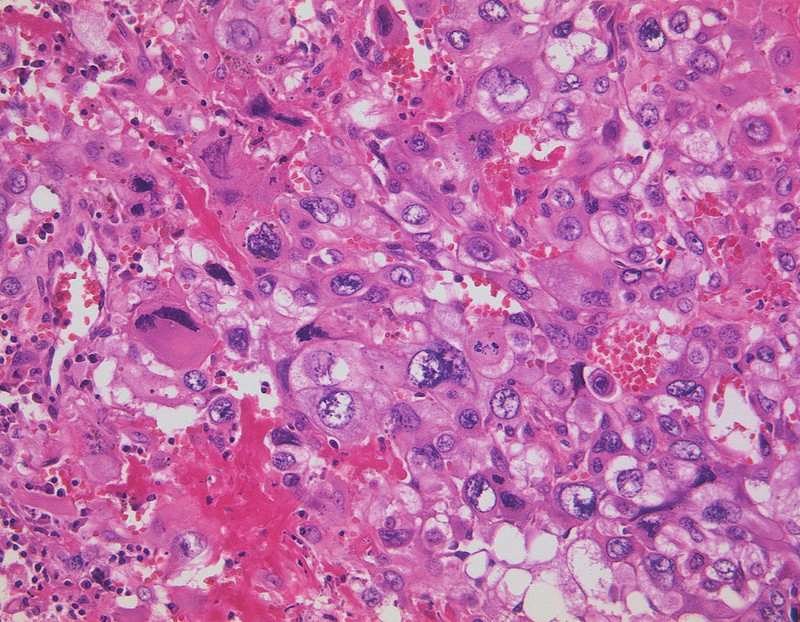
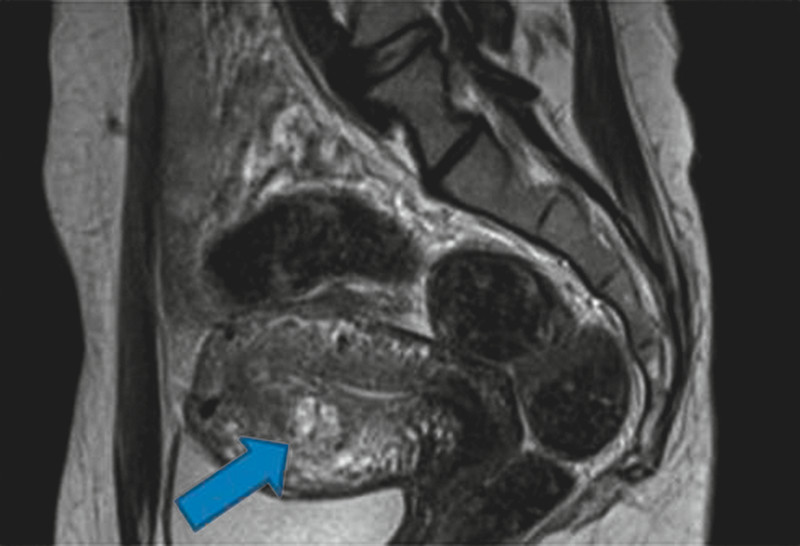
Gestational trophoblastic diseases (GTD) are a group of pregnancy-related disorders representing rare human tumours. They encompass premalignant disorders including complete (CHM), partial hydatidiform mole (PHM), exaggerated placental site (EPS), and placental-site nodule (PSN) as well as malignant disorders (also known as "gestational trophoblastic neoplasia [GTN]") including invasive mole, choriocarcinoma (CC), placenta-site trophoblastic tumour (PSTT), and epitheloid trophoblastic tumours (ETT) (Fig. 1). Originally, GTD develop from abnormal proliferation of trophoblastic tissue and form botryoid arranged vesicles. Premalignant moles are usually treated by suction curettage while persistent and recurrent moles and malignant forms require systemic therapy with methotrexate or combination chemotherapy consisting of etoposide, actimomycin D, methotrexate, vincristine, and cyclophosphamide (EMA-CO). β-human chorion gonadotropin (β-hCG) plays a crucial role in diagnosis and monitoring therapeutic effects. Since the definitive diagnosis cannot be obtained by histology in most cases, persistent or recurrent disease is diagnosed by elevated or persistent serum levels of β-hCG. While curing rates are described to be as high as 98 %, GTD may initially present, recur, or end up as a metastasising systemic disease. This underlines the importance of a regular and consistent follow-up after treatment.
Gestationsbedingte Trophoblasterkrankungen (GTE) gehören zu der Gruppe seltener menschlicher Tumoren, die im Rahmen einer Schwangerschaft entstehen. Diese Gruppe umfasst prämaligne Veränderungen wie Blasenmole und Partialmole, hyperplastische Implantationsstelle des Plazentabetts (exaggerated placental site, EPS) und Plazentabettknötchen (placental site nodule, PSN) sowie maligne Erkrankungen (auch gestationsbedingte Trophoblastneoplasien [GTN] genannt) wie invasive Molen, Chorionkarzinom, Plazentabetttumor (placental site trophoblastic tumor, PSTT) und epitheloider Trophoblasttumor (ETT) (Abb. 1). Die Entstehung von GTE ist durch die abnorme Proliferation von Trophoblastzellen gekennzeichnet, die traubenförmig angeordnete Bläschen bilden. Prämaligne Molen werden zumeist mit Saugkürettage therapiert. Die Behandlung persistierender und rezidivierender Molen sowie maligner Formen besteht aus einer systemischen Therapie mit Methotrexat oder einer Kombinationschemotherapie aus Etoposid, Actinomycin-D, Methotrexat, Vincristin, und Cyclophosphamid (EMA-CO). β-humanes Choriongonadotropin (β-hCG) spielt eine wichtige Rolle bei der Diagnose und Kontrolle der Therapie. Da eine histologische Untersuchung in den meisten Fällen keine endgültige Diagnose liefert, beruht die Diagnose von Persistenz und Rezidiv auf erhöhten (persistierenden) Serumkonzentrationen von β-hCG. Obwohl die in der Literatur angegebenen Heilungsraten hoch sind mit bis zu 98 %, können GTE nach dem ersten Auftreten rekurrieren oder in eine systemische Erkrankung mit Metastasierung übergehen. Dies unterstreicht die Bedeutung einer regelmäßigen und konsequenten Nachsorge.
Keywords: gestational neoplasia; gestational trophoblastic disease; human chorion gonadotropin; hydatidiform moles; molar pregnancy.
Conflict of interest statement
Figures
References
-
- Seckl M J, Sebire N J, Berkowitz R S. Gestational trophoblastic disease. Lancet. 2010;376:717–729. - PubMed
-
- Palmer J R. Advances in the epidemiology of gestational trophoblastic disease. J Reprod Med. 1994;39:155–162. - PubMed
-
- Ngan S, Seckl M J. Gestational trophoblastic neoplasia management: an update. Curr Opin Oncol. 2007;19:486–491. - PubMed
-
- Seckl M J, Fisher R A, Salerno G. et al. Choriocarcinoma and partial hydatidiform moles. Lancet. 2000;356:36–39. - PubMed
Publication types
LinkOut - more resources
Full Text Sources
Other Literature Sources
Research Materials