

Cirrhotic cardiomyopathy
- PMID: 26556983
- PMCID: PMC4631957
- DOI: 10.3748/wjg.v21.i41.11502
Cirrhotic cardiomyopathy
Abstract
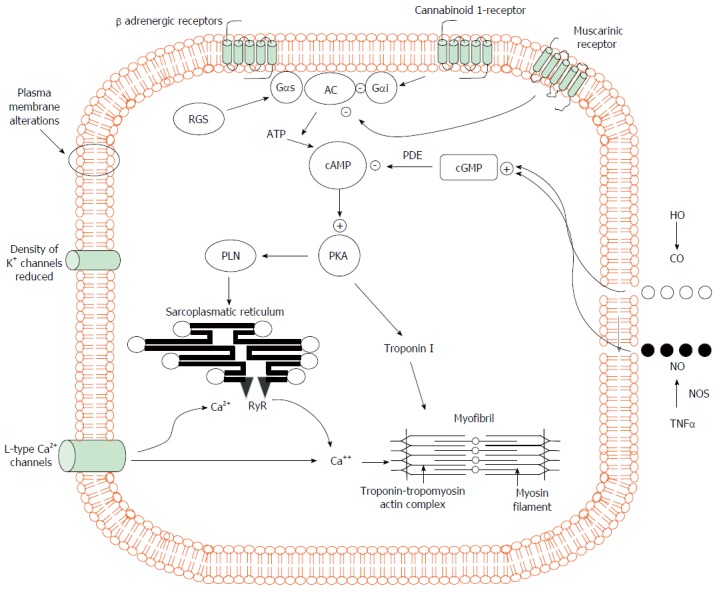
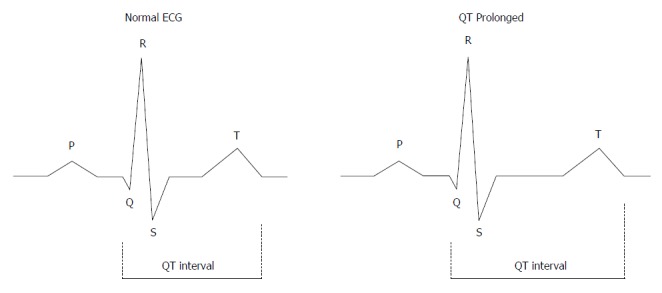
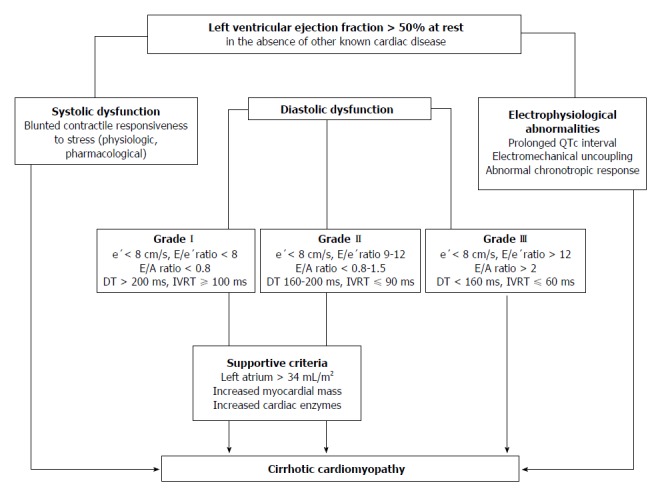
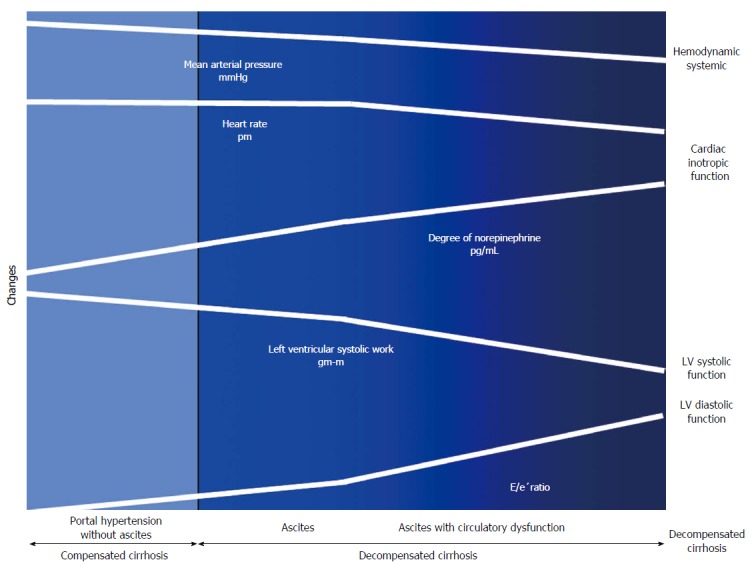
During the course of cirrhosis, there is a progressive deterioration of cardiac function manifested by the disappearance of the hyperdynamic circulation due to a failure in heart function with decreased cardiac output. This is due to a deterioration in inotropic and chronotropic function which takes place in parallel with a diastolic dysfunction and cardiac hypertrophy in the absence of other known cardiac disease. Other findings of this specific cardiomyopathy include impaired contractile responsiveness to stress stimuli and electrophysiological abnormalities with prolonged QT interval. The pathogenic mechanisms of cirrhotic cardiomyopathy include impairment of the b-adrenergic receptor signalling, abnormal cardiomyocyte membrane lipid composition and biophysical properties, ion channel defects and overactivity of humoral cardiodepressant factors. Cirrhotic cardiomyopathy may be difficult to determine due to the lack of a specific diagnosis test. However, an echocardiogram allows the detection of the diastolic dysfunction and the E/e' ratio may be used in the follow-up progression of the illness. Cirrhotic cardiomyopathy plays an important role in the pathogenesis of the impairment of effective arterial blood volume and correlates with the degree of liver failure. A clinical consequence of cardiac dysfunction is an inadequate cardiac response in the setting of vascular stress that may result in renal hypoperfusion leading to renal failure. The prognosis is difficult to establish but the severity of diastolic dysfunction may be a marker of mortality risk. Treatment is non-specific and liver transplantation may normalize the cardiac function.
Keywords: Arterial blood volume; Cirrhosis; Cirrhotic cardiomyopathy; E/e’ ratio; Hepatorenal syndrome; Inotropic heart dysfunction; Left ventricular diastolic dysfunction; Liver failure.
Figures
References
-
- Murray JF, Dawson AM, Sherlock S. Circulatory changes in chronic liver disease. Am J Med. 1958;24:358–367. - PubMed
-
- Bernardi M, Rubboli A, Trevisani F, Cancellieri C, Ligabue A, Baraldini M, Gasbarrini G. Reduced cardiovascular responsiveness to exercise-induced sympathoadrenergic stimulation in patients with cirrhosis. J Hepatol. 1991;12:207–216. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
