

Do vasopressin V2 receptor antagonists benefit cirrhotics with refractory ascites?
- PMID: 26556988
- PMCID: PMC4631962
- DOI: 10.3748/wjg.v21.i41.11584
Do vasopressin V2 receptor antagonists benefit cirrhotics with refractory ascites?
Abstract
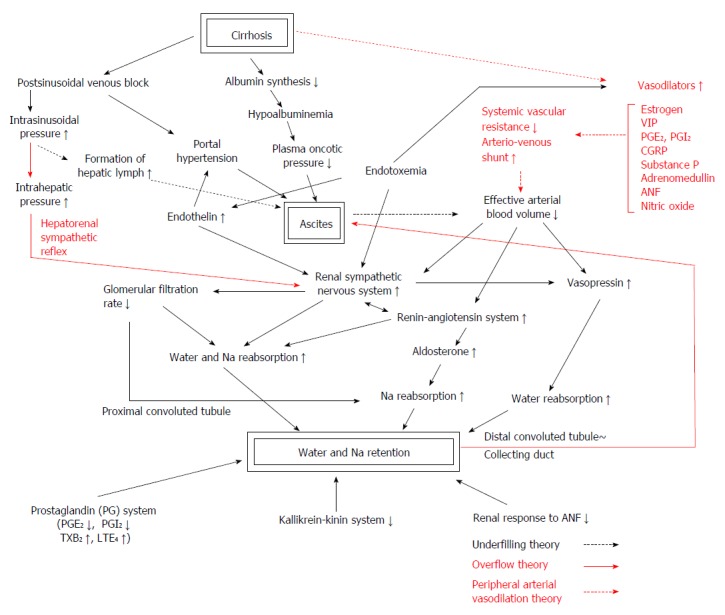
Hyponatremia is a frequent complication of advanced cirrhosis with ascites associated with increased morbidity and mortality. It is caused by an impairment in the renal capacity to eliminate solute-free water and is considered to be related to persistent secretion of vasopressin despite low serum osmolality. This nonosmotic release of vasopressin is mediated by the autonomic nervous system, which senses the underfilling of arterial vascular component. This reduction of effective arterial blood volume is closely related to the development of ascites. Although the short-time effects of vasopressin V2 receptor antagonists (vaptans) on hyponatremia and ascites have been repeatedly reported, their effects on the long-term management of cirrhotic ascites have not been established yet. Considering that their effects on water diuresis and their safety are limited by severe underfilling state of patients, cautious approaches with adequate monitoring are needed to advanced cirrhosis. Proper indication, adequate doses and new possibility of combination therapy should be explored in the future controlled study. As hyponatremia is frequent obstacle to ascites management, judicious combination with low-dose diuretics may decrease the incidence of refractory ascites. Although vaptans show much promise in the treatment of advanced cirrhosis, the problem of high cost should be solved for the future.
Keywords: Ascites; Hyponatremia; Liver cirrhosis; Pathophysiology; V2 receptor antagonist.
Figures
Similar articles
-
Hyponatremia in cirrhosis: pathophysiology and management.World J Gastroenterol. 2015 Mar 21;21(11):3197-205. doi: 10.3748/wjg.v21.i11.3197. World J Gastroenterol. 2015. PMID: 25805925 Free PMC article. Review.
-
The treatment of vasopressin V2-receptor antagonists in cirrhosis patients with ascites: a meta-analysis of randomized controlled trials.BMC Gastroenterol. 2015 Jun 9;15:65. doi: 10.1186/s12876-015-0297-z. BMC Gastroenterol. 2015. PMID: 26054761 Free PMC article.
-
[Current options of treatment of hyponatremia].Vnitr Lek. 2016 Winter;62 Suppl 6:97-101. Vnitr Lek. 2016. PMID: 28124939 Czech.
-
[Management of ascites in cirrhotic patients].Nihon Shokakibyo Gakkai Zasshi. 2017;114(1):27-34. doi: 10.11405/nisshoshi.114.27. Nihon Shokakibyo Gakkai Zasshi. 2017. PMID: 28070092 Review. Japanese. No abstract available.
-
Pathophysiology of ascites and dilutional hyponatremia: contemporary use of aquaretic agents.Ann Hepatol. 2007 Oct-Dec;6(4):214-21. Ann Hepatol. 2007. PMID: 18007550 Review.
Cited by
-
Refractory ascites-the contemporary view on pathogenesis and therapy.PeerJ. 2019 Oct 15;7:e7855. doi: 10.7717/peerj.7855. eCollection 2019. PeerJ. 2019. PMID: 31637125 Free PMC article.
-
Management of refractory cirrhotic ascites: challenges and solutions.Hepat Med. 2018 Jul 3;10:55-71. doi: 10.2147/HMER.S136578. eCollection 2018. Hepat Med. 2018. PMID: 30013405 Free PMC article. Review.
-
Water, electrolyte, acid-base, and trace elements alterations in cirrhotic patients.Int Urol Nephrol. 2018 Jan;50(1):81-89. doi: 10.1007/s11255-017-1614-y. Epub 2017 Jun 12. Int Urol Nephrol. 2018. PMID: 28608260 Review.
-
Efficacy of tolvaptan for the patients with advanced hepatocellular carcinoma.World J Gastroenterol. 2017 Aug 7;23(29):5379-5385. doi: 10.3748/wjg.v23.i29.5379. World J Gastroenterol. 2017. PMID: 28839438 Free PMC article.
-
Predicting short-term survival after liver transplantation on eight score systems: a national report from China Liver Transplant Registry.Sci Rep. 2017 Feb 13;7:42253. doi: 10.1038/srep42253. Sci Rep. 2017. PMID: 28198820 Free PMC article.
References
-
- Ginès P, Guevara M. Hyponatremia in cirrhosis: pathogenesis, clinical significance, and management. Hepatology. 2008;48:1002–1010. - PubMed
-
- Lehrich RW, Ortiz-Melo DI, Patel MB, Greenberg A. Role of vaptans in the management of hyponatremia. Am J Kidney Dis. 2013;62:364–376. - PubMed
-
- Vaamonde C. Renal water handling in liver disease. In: Epstein M, editor. The Kidney in Liver Disease. 4th ed. Philadelphia: Hanley and Belfus Inc; 1996. pp. 33–74.
-
- Levy M. Pathophysiology of ascites formation. In: Epstein M, editor. The Kidney in Liver Disease. 3rd ed. Baltimore: Williams and Wilkins; 1988. pp. 209–243.
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
Miscellaneous
