

Recurrent respiratory tract infections in children - analysis of immunological examinations
- PMID: 26557030
- PMCID: PMC4637391
- DOI: 10.5114/ceji.2015.52830
Recurrent respiratory tract infections in children - analysis of immunological examinations
Abstract
Background: Paediatric respiratory tract infections are among the most common reasons for preschool and school absences and visits to physicians. The disease mainly involves the upper respiratory tract and is associated with fever, cough, sore throat, and running nose. Children with recurrent respiratory infections (RRI), which are defined as more than six serious diseases a year, are a difficult diagnostic challenge. The aim of this study was to assess immunological deviations in laboratory tests performed in children with RRI.
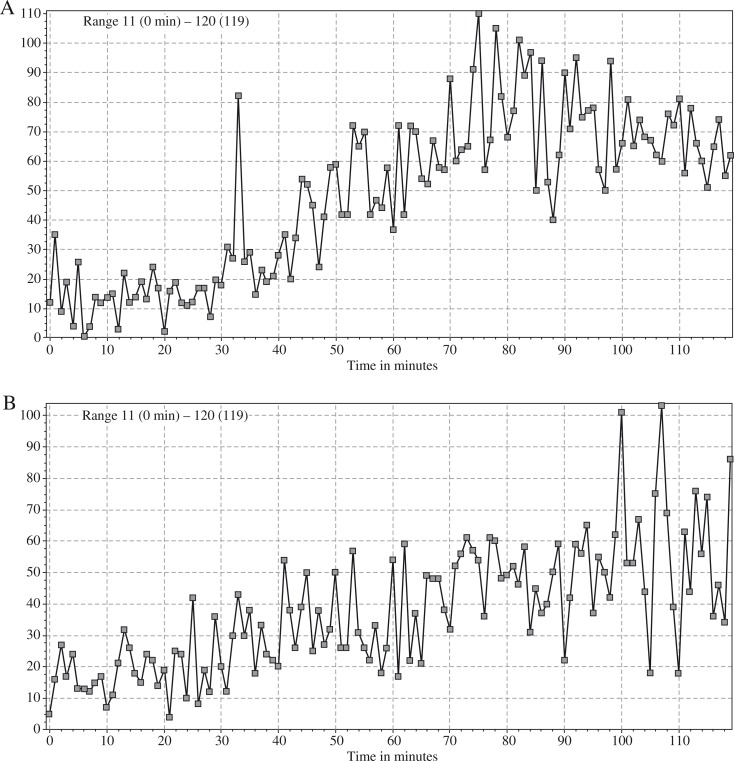
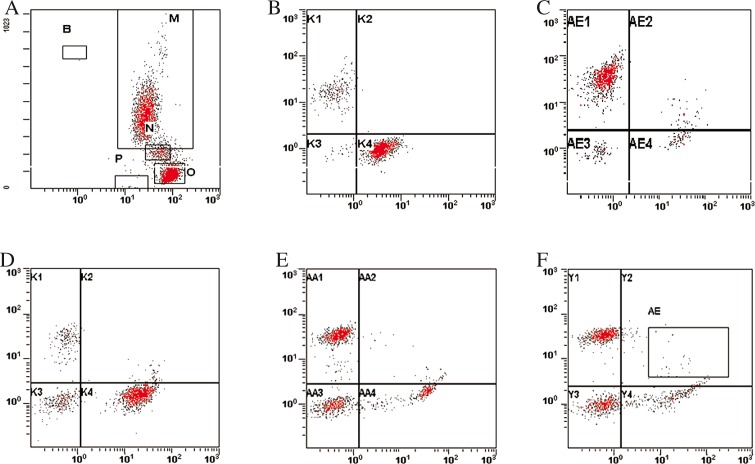
Material and methods: In the retrospective study 25 children suffering from recurrent respiratory tract infection, aged 4.1 ±2.3 years, 13 boys and 12 girls, were involved. For all children chemiluminescence of granulocytes and immunophenotyping of lymphocytes from peripheral blood were examined. An immunophenotype of peripheral blood lymphocytes involved evaluation of T cell, B cells, and NK cells, examined with flow cytometry.
Results: Eleven of the studied children had decreased chemiluminescent response to stimulants, normal response was found for nine children, and five children had an increased result of the test. Five of the 25 children had decreased B cells number, and five had decreased number of T cells including decrease of CD4, as well as CD8 positive cells. Children with decreased chemiluminescence had more frequent neutropaenia than children with normal or increased chemiluminescent response, p < 0.05 (exact Fisher test).
Conclusions: Recurrent respiratory tract infection could be associated with improper neutrophils response to pathogens, and immunological examination should be performed to find the reason for the increased number of infections in a year.
Keywords: chemiluminescence; immunological disturbances; immunophenotyping; recurrent respiratory tract infection.
Figures
References
-
- Kilic SS. Recent Advances in Pediatrics. New Delhi: Jaypee Brothers Medical Publishers; 2004. Recurrent respiratory tract infection; pp. 1–18.
-
- Jenesak M, Ciljakova M, Rennerova Z, et al. Recurrent Respiratory Infections in Children – Definition, Diagnostic Approach, Treatment and Prevention. In: Martin-Loeches I, editor. Bronchitis. InTech; 2011. pp. 119–148.
-
- Stokłosa T. Niedobory odporności. In: Gołąb J, Jakóbisiak M, Lasek W, Stokłosa T, editors. Immunologia. Warsaw: PWN; 2007. pp. 398–426.
-
- Raport of WHO Scientific Group. Primary immunodeficiency diseases. Clin Exp Immunol. 1997;109:26–28. - PubMed
-
- Kowalska M, Kowalska H, Zawadzka-Głos L, et al. Dysfunction of peripheral blood granulocyte oxidative metabolism in children with upper recurrent respiratory tract infections. Int J Pediatr Othorhinolaryngol. 2003;67:365–371. - PubMed
LinkOut - more resources
Full Text Sources
Other Literature Sources
Research Materials