

Complications of needle thoracostomy: A comprehensive clinical review
- PMID: 26557486
- PMCID: PMC4613415
- DOI: 10.4103/2229-5151.164939
Complications of needle thoracostomy: A comprehensive clinical review
Abstract
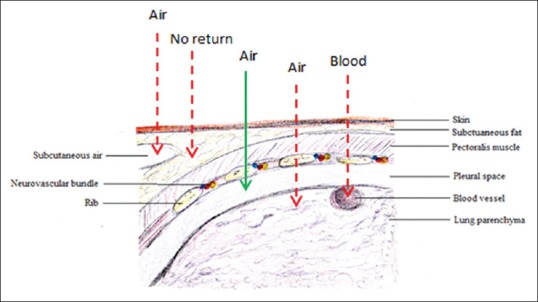
Needle thoracostomy (NT) is a valuable adjunct in the management of tension pneumothorax (tPTX), a life-threatening condition encountered mainly in trauma and critical care environments. Most commonly, needle thoracostomies are used in the prehospital setting and during acute trauma resuscitation to temporize the affected individuals prior to the placement of definitive tube thoracostomy (TT). Because it is both an invasive and emergent maneuver, NT can be associated with a number of potential complications, some of which may be life-threatening. Due to relatively common use of this procedure, it is important that healthcare providers are familiar, and ready to deal with, potential complications of NT.
Keywords: Complications; emergent chest decompression; needle thoracostomy; tension pneumothorax.
Conflict of interest statement
Figures



References
-
- Butler KL, Best IM, Weaver WL, Bumpers HL. Pulmonary artery injury and cardiac tamponade after needle decompression of a suspected tension pneumothorax. J Trauma. 2003;54:610–1. - PubMed
-
- Carney M, Ravin CE. Intercostal artery laceration during thoracocentesis: Increased risk in elderly patients. Chest. 1979;75:520–2. - PubMed
LinkOut - more resources
Full Text Sources
Other Literature Sources
Research Materials
