

Combined radiological-endoscopic management of difficult bile duct stones: 18-year single center experience
- PMID: 26557890
- PMCID: PMC4622282
- DOI: 10.1177/1756283X15587483
Combined radiological-endoscopic management of difficult bile duct stones: 18-year single center experience
Abstract
Objectives: Clinical evidence regarding radiological-endoscopic management of intrahepatic bile duct stones is currently lacking. Our aim is to report our 18-year experience in combined radiological-endoscopic management of intrahepatic difficult bile duct stones.
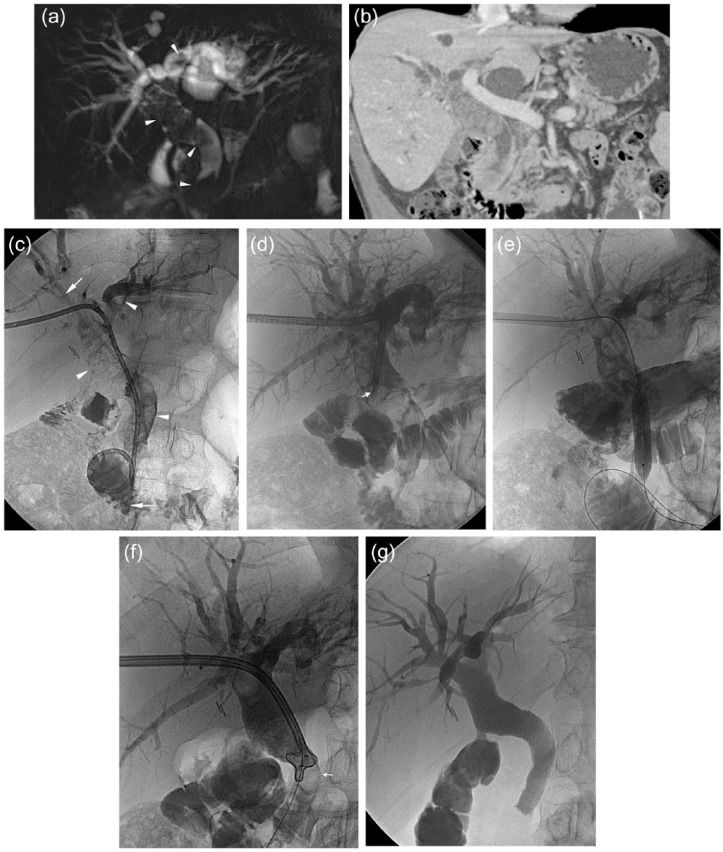
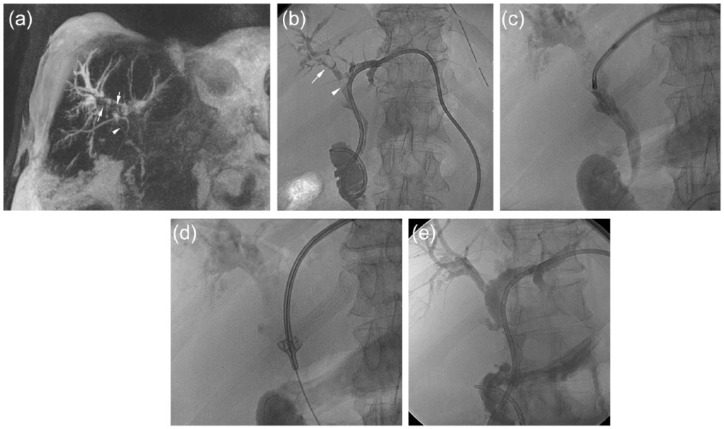
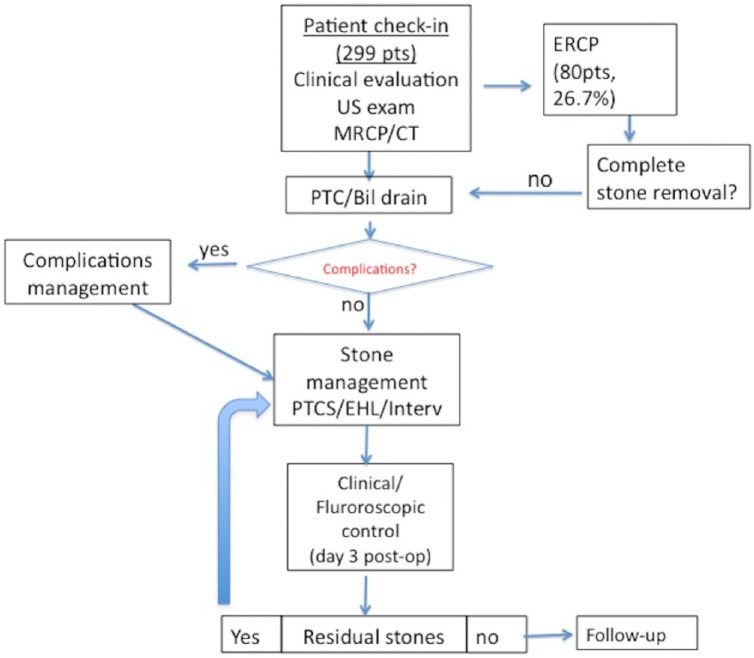
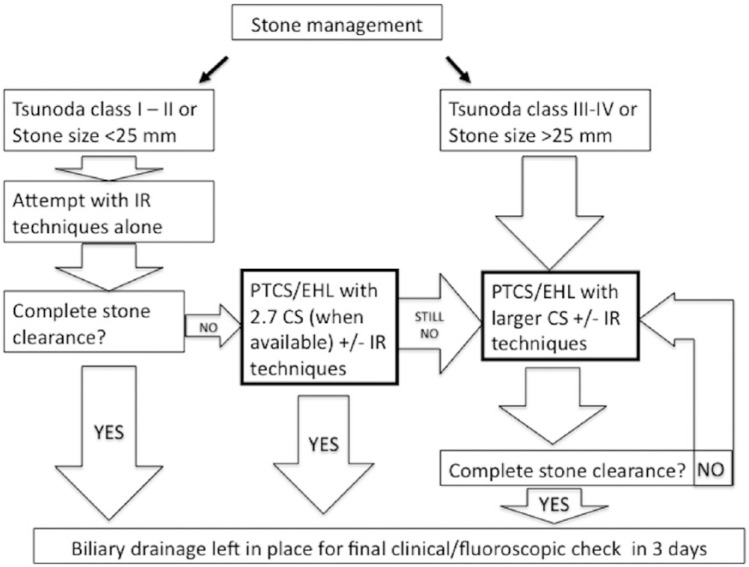
Methods: From June 1994 to June 2012, 299 symptomatic patients with difficult bile duct stones were admitted to our institution. Percutaneous transhepatic cholangiography (PTC)/biliary drainage/s was performed, dilating the PTC track to 10 or 16 French within 3-7 days. Afterward we carried out percutaneous transhepatic cholangioscopy (PTCS) with electrohydraulic lithotripsy (EHL) and/or interventional radiology techniques. Follow up was made with clinical/laboratory tests and ultrasound (US). We retrospectively analyzed our radiological-endoscopic approach and reported our technical and clinical outcomes.
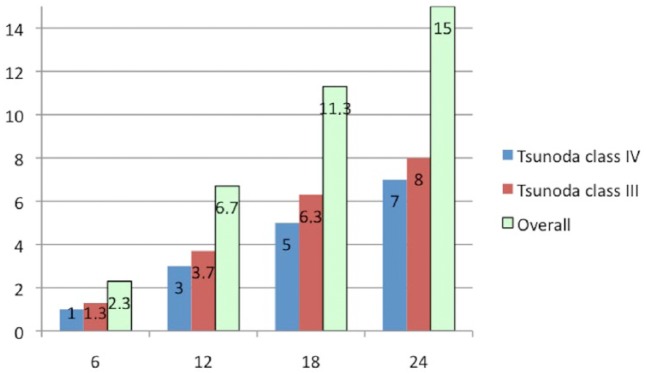
Results: Complete stone clearance was achieved in 298 patients after a maximum of 4 consecutive sessions. Most patients (64.6%) were treated with PTCS/EHL alone, while the remaining with radiological techniques alone (26%) or a combination of both techniques (13.3%). Recurrence of stones occurred in 45 cases (15%, Tsunoda class III and class IV) within 2 years and were successfully retreated. Major adverse events were: 5 (1.6%) cases of massive bleeding that required embolisation, 2 (0.66%) perforations of the common bile duct and 31 cases (10.3%) of acute cholangitis managed with medical therapy or intervention.
Conclusion: After 18 years of experience we demonstrated that our combined radiological-endoscopic approach to 'difficult bile duct stones' may result in both immediate and long-term clearance of stones with a low rate of adverse events.
Keywords: bile ducts; biliary stones; cholangiography; endoscopy; lithotripsy.
Conflict of interest statement
Figures
Similar articles
-
Electrohydraulic lithotripsy in 111 patients: a safe and effective therapy for difficult bile duct stones.Am J Gastroenterol. 2004 Dec;99(12):2330-4. doi: 10.1111/j.1572-0241.2004.40251.x. Am J Gastroenterol. 2004. PMID: 15571578
-
Treatment of bile duct stones: value of laser lithotripsy delivered via percutaneous endoscopy.Eur Radiol. 1996;6(5):734-40. doi: 10.1007/BF00187681. Eur Radiol. 1996. PMID: 8934142
-
Outcomes of Single-Operator Cholangioscopy-Guided Lithotripsy in Patients with Difficult Biliary and Pancreatic Stones.GE Port J Gastroenterol. 2019 Mar;26(2):105-113. doi: 10.1159/000488508. Epub 2018 May 16. GE Port J Gastroenterol. 2019. PMID: 30976615 Free PMC article.
-
Recent advances in endoscopic management of difficult bile duct stones.Dig Endosc. 2013 Jul;25(4):376-85. doi: 10.1111/den.12118. Epub 2013 May 8. Dig Endosc. 2013. PMID: 23650878 Review.
-
Electrohydraulic lithotripsy combined with laparoscopy and endoscopy for managing difficult biliary stones.Surg Laparosc Endosc. 1993 Oct;3(5):398-402. Surg Laparosc Endosc. 1993. PMID: 8261270 Review.
Cited by
-
Safety, diagnostic accuracy and therapeutic efficacy of digital single-operator cholangioscopy.United European Gastroenterol J. 2018 Jul;6(6):902-909. doi: 10.1177/2050640618764943. Epub 2018 Mar 8. United European Gastroenterol J. 2018. PMID: 30023068 Free PMC article.
-
Strategies of minimally invasive treatment for intrahepatic and extrahepatic bile duct stones.Front Med. 2017 Dec;11(4):576-589. doi: 10.1007/s11684-017-0536-5. Epub 2017 Aug 12. Front Med. 2017. PMID: 28801889
-
Effectiveness and complication rates of percutaneous transhepatic fluoroscopy-guided management of common bile duct stones: a single-arm meta-analysis.Eur Radiol. 2023 Nov;33(11):7398-7407. doi: 10.1007/s00330-023-09846-z. Epub 2023 Jun 16. Eur Radiol. 2023. PMID: 37326663
-
Advances in Therapeutic Cholangioscopy.Gastroenterol Res Pract. 2016;2016:5249152. doi: 10.1155/2016/5249152. Epub 2016 Jun 15. Gastroenterol Res Pract. 2016. PMID: 27403156 Free PMC article. Review.
-
PERcutaneous transhepatic CHOLangioscopy using a new single-operator short cholangioscope (PERCHOL): European feasibility study.Dig Endosc. 2024 Jun;36(6):719-725. doi: 10.1111/den.14697. Epub 2023 Oct 31. Dig Endosc. 2024. PMID: 37772447 Free PMC article.
References
-
- Buxbaum J. (2013) Modern management of common bile duct stones. Gastrointest Endosc Clin N Am 23: 251–275. - PubMed
-
- Chen C., Huang M., Yang J., Yang C., Yeh Y., Wu H., et al. (2005) Reappraisal of percutaneous transhepatic cholangioscopic lithotomy for primary hepatolithiasis. Surg Endosc 19: 505–509. - PubMed
-
- Cheon Y., Cho Y., Moon J., Lee J., Shim C. (2009) Evaluation of long-term results and recurrent factors after operative and nonoperative treatment for hepatolithiasis. Surgery 146: 843–853. - PubMed
-
- Erim T., Shiroky J., Pleskow D. (2013) Cholangioscopy: the biliary tree never looked so good! Curr Opin Gastroenterol 29: 501–508. - PubMed
-
- García-Vila J., Redondo-Ibáñez M., Díaz-Ramón C. (2004) Balloon sphincteroplasty and transpapillary elimination of bile duct stones: 10 years’ experience. AJR Am J Roentgenol 182: 1451–1458. - PubMed
LinkOut - more resources
Full Text Sources
