

Accidental invisible intrathoracic disseminated pT4-M1a: a distinct lung cancer with favorable prognosis
- PMID: 26557992
- PMCID: PMC4522477
- DOI: 10.3978/j.issn.2072-1439.2015.05.19
Accidental invisible intrathoracic disseminated pT4-M1a: a distinct lung cancer with favorable prognosis
Erratum in
-
Erratum to accidental invisible intrathoracic disseminated pT4-M1a: a distinct lung cancer with favorable prognosis.J Thorac Dis. 2015 Sep;7(9):E394. doi: 10.3978/j.issn.2072-1439.2015.10.01. J Thorac Dis. 2015. PMID: 26543638 Free PMC article.
Abstract
Objective: In the 7(th) edition of the TNM classification of malignant tumors, the prognosis for pT4-M1a stage IV lung cancer is better than for stage pIIIB. Subgroups of lung cancer patients who underwent incomplete resection (R1/R2) have a favorable prognosis. This study compares the prognosis between cases of invisible local residual disease and intrathoracic disseminated pT4-M1aIV.
Methods: Patient characteristics and histological and molecular profiles were retrospectively collected for lung cancer patients who underwent resection intended to be curative but were accidentally incomplete. All patients were divided into either a local residual group or an intrathoracic disseminated pT4M1a group. Progression-free survival (PFS) and overall survival (OS) were evaluated by Kaplan-Meier and Cox regression models.
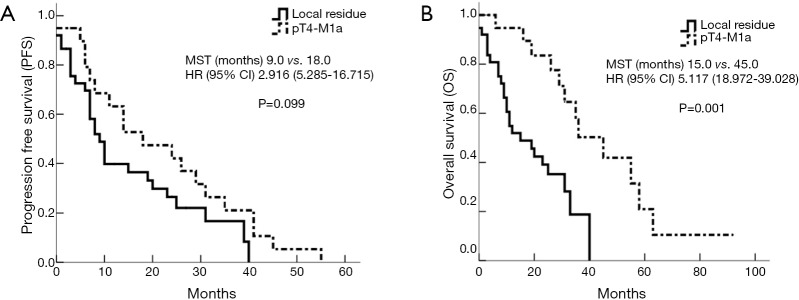
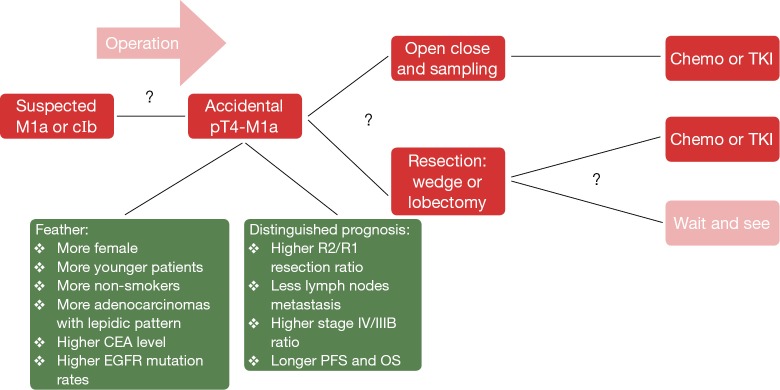
Results: In total, 1,483 consecutive lung cancer patients receiving thoracotomies at Guangdong Lung Cancer Institute were retrospectively analyzed. Fifty-eight patients receiving incomplete resections (R1/R2) were enrolled, including 38 patients with local residual cancer (2.6% of all patients) and 20 patients with disseminated pM1a (1.3%). Patient characteristics, and histological and molecular profiles of the two groups were different. Compared to the local residual group, the disseminated pT4-M1a group contained more females (P=0.002), more patients younger than 60 years of age (P=0.028), more non-smokers (P=0.037), more adenocarcinomas (20/20 vs. 20/38, P<0.001), more adenocarcinomas with lepidic pattern (11/20 vs. 4/38, P<0.001), higher carcinoembryonic antigen (CEA) levels (P=0.06), higher epidermal growth factor receptor (EGFR) mutation rates (16/20 vs. 7/38, P<0.001), a higher R2/R1 resection ratio (P=0.013), a higher advanced stage IV/IIIB ratio (P<0.001), but fewer lymph node metastases (P=0.013). Median PFS for the local residual and disseminated pT4-M1a groups was 9.0 and 18.0 months, respectively [95% confidence interval (CI), 5.285-16.715; P =0.099]. Median OS was 15.0 and 45.0 months, respectively (95% CI, 18.972-39.028; P=0.001). Cox regression analysis revealed that group (local residual vs. disseminated pT4-M1a) was the only independent prognostic factor (P=0.044) for OS.
Conclusions: Accidental invisible intrathoracic disseminated pT4-M1a may be a distinct lung cancer subtype with a favorable prognosis. The prolonged PFS and OS might reflect the natural history of this distinct subtype, together with a favorable response to EGFR tyrosine kinase inhibitors (EGFR-TKI). For asymptomatic and slow-growing accidental pT4-M1a disease, the role of a wait-and-see strategy and the appropriate timing of systemic treatment require further investigation.
Keywords: Lung cancer; accidental invisible pT4-M1a; incomplete resection; prognosis.
Conflict of interest statement
Figures
Similar articles
-
Erratum to accidental invisible intrathoracic disseminated pT4-M1a: a distinct lung cancer with favorable prognosis.J Thorac Dis. 2015 Sep;7(9):E394. doi: 10.3978/j.issn.2072-1439.2015.10.01. J Thorac Dis. 2015. PMID: 26543638 Free PMC article.
-
Effect of epidermal growth factor receptor gene mutation on the prognosis of pathological stage II-IIIA (8th edition TNM classification) primary lung cancer after curative surgery.Lung Cancer. 2021 Dec;162:128-134. doi: 10.1016/j.lungcan.2021.11.002. Epub 2021 Nov 8. Lung Cancer. 2021. PMID: 34775216
-
Prognostic impact of M descriptors of the 8th edition of TNM classification of lung cancer.J Thorac Dis. 2017 Mar;9(3):685-691. doi: 10.21037/jtd.2017.03.106. J Thorac Dis. 2017. PMID: 28449476 Free PMC article.
-
Effect of smoking status on progression-free and overall survival in non-small cell lung cancer patients receiving erlotinib or gefitinib: a meta-analysis.J Clin Pharm Ther. 2015 Dec;40(6):661-71. doi: 10.1111/jcpt.12332. Epub 2015 Nov 17. J Clin Pharm Ther. 2015. PMID: 26573867
-
New horizons in non-small-cell lung cancer patients with ipsilateral pleural dissemination (M1a): review of the literature.Ann Transl Med. 2021 Jun;9(11):959. doi: 10.21037/atm-20-6188. Ann Transl Med. 2021. PMID: 34350274 Free PMC article. Review.
Cited by
-
[Observation - An Favorable Option Forthoracic Dissemination Patients with Lung Adenocarcinoma or Squamous Carcinoma].Zhongguo Fei Ai Za Zhi. 2018 Apr 20;21(4):303-309. doi: 10.3779/j.issn.1009-3419.2018.04.14. Zhongguo Fei Ai Za Zhi. 2018. PMID: 29587911 Free PMC article. Chinese.
-
Surgical Resection of Primary Tumors Provides Survival Benefits for Lung Cancer Patients With Unexpected Pleural Dissemination.Front Surg. 2021 Jun 23;8:679565. doi: 10.3389/fsurg.2021.679565. eCollection 2021. Front Surg. 2021. PMID: 34250008 Free PMC article.
-
Recursive partitioning analysis of patients with oligometastatic non-small cell lung cancer: a retrospective study.BMC Cancer. 2019 Nov 6;19(1):1051. doi: 10.1186/s12885-019-6216-x. BMC Cancer. 2019. PMID: 31694572 Free PMC article.
-
ASO Author Reflections: Lung Adenocarcinoma with Accidental Invisible Pleural Dissemination Lesions: Wait-and-See Strategy for Tumors with Indolent Biologic Characteristics.Ann Surg Oncol. 2020 Oct;27(10):3819-3820. doi: 10.1245/s10434-020-08402-z. Epub 2020 Mar 27. Ann Surg Oncol. 2020. PMID: 32221740 No abstract available.
-
Rab11a promotes proliferation and invasion through regulation of YAP in non-small cell lung cancer.Oncotarget. 2017 Apr 25;8(17):27800-27811. doi: 10.18632/oncotarget.15359. Oncotarget. 2017. PMID: 28468127 Free PMC article.
References
-
- Siegel RL, Miller KD, Jemal A. Cancer statistics, 2015. CA Cancer J Clin 2015;65:5-29. - PubMed
-
- Zheng H, Hu XF, Jiang GN, et al. Define relative incomplete resection by highest mediastinal lymph node metastasis for non-small cell lung cancers: rationale based on prognosis analysis. Lung Cancer 2011;72:348-54. - PubMed
-
- Verhagen AF, Schoenmakers MC, Barendregt W, et al. Completeness of lung cancer surgery: is mediastinal dissection common practice? Eur J Cardiothorac Surg 2012;41:834-8. - PubMed
-
- Postmus PE, Brambilla E, Chansky K, et al. The IASLC Lung Cancer Staging Project: proposals for revision of the M descriptors in the forthcoming (seventh) edition of the TNM classification of lung cancer. J Thorac Oncol 2007;2:686-93. - PubMed
LinkOut - more resources
Full Text Sources
Research Materials
Miscellaneous