

Metabolic syndrome, obesity and kidney stones
- PMID: 26558034
- PMCID: PMC4442970
- DOI: 10.1016/j.aju.2012.04.005
Metabolic syndrome, obesity and kidney stones
Abstract
Objectives: To give a comprehensive and focused overview on the current knowledge of the causal relations of metabolic syndrome and/or central obesity with kidney stone formation.
Methods: Previous reports were reviewed using PubMed, with a strict focus on the keywords (single or combinations thereof): urolithiasis, nephrolithiasis, kidney stones, obesity, metabolic syndrome, bariatric surgery, calcium oxalate stones, hyperoxaluria, insulin resistance, uric acid stones, acid-base metabolism.
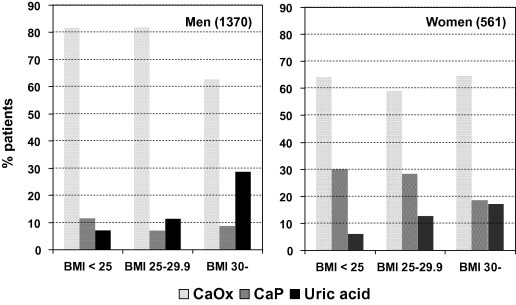
Results: Obesity (a body mass index, BMI, of >30 kg/m(2)) affects 10-27% of men and up to 38% of women in European countries. Worldwide, >300 million people are estimated to be obese. Epidemiologically, a greater BMI, greater weight, larger waist circumference and major weight gain are independently associated with an increased risk of renal stone formation, both for calcium oxalate and uric acid stone disease.
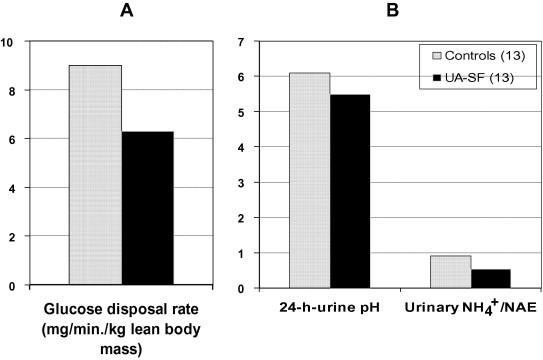
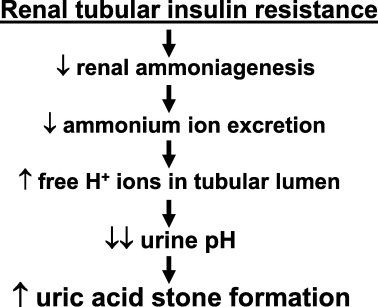
Conclusions: There are two distinct metabolic conditions accounting for kidney stone formation in patients with metabolic syndrome/central obesity. (i) Abdominal obesity predisposes to insulin resistance, which at the renal level causes reduced urinary ammonium excretion and thus a low urinary pH; the consequence is a greater risk of uric acid stone formation. (ii) Bariatric surgery, the only intervention that facilitates significant weight loss in morbidly obese people, carries a greater risk of calcium oxalate nephrolithiasis. The underlying pathophysiological mechanisms are profound enteric hyperoxaluria due to intestinal binding of calcium by malabsorbed fatty acids, and severe hypocitraturia due to soft or watery stools, which lead to chronic bicarbonate losses and intracellular metabolic acidosis.
Keywords: BMI, body mass index; Bariatric surgery; CaOx, calcium oxalate; Enteric hyperoxaluria; HDL, high-density lipoprotein; Hypocitraturia; Metabolic syndrome; Obesity; RYGB, Roux-en-Y-gastric bypass; UA, uric acid; Uric acid stones.
Figures

Similar articles
-
Clinical and biochemical profile of patients with "pure" uric acid nephrolithiasis compared with "pure" calcium oxalate stone formers.Urol Res. 2007 Oct;35(5):247-51. doi: 10.1007/s00240-007-0109-1. Epub 2007 Sep 6. Urol Res. 2007. PMID: 17786420
-
Dietary treatment of urinary risk factors for renal stone formation. A review of CLU Working Group.Arch Ital Urol Androl. 2015 Jul 7;87(2):105-20. doi: 10.4081/aiua.2015.2.105. Arch Ital Urol Androl. 2015. PMID: 26150027 Review.
-
Effect of being overweight on urinary metabolic risk factors for kidney stone formation.Nephrol Dial Transplant. 2015 Apr;30(4):607-13. doi: 10.1093/ndt/gfu350. Epub 2014 Oct 31. Nephrol Dial Transplant. 2015. PMID: 25362001
-
Association of metabolic syndrome traits and severity of kidney stones: results from a nationwide survey on urolithiasis in Japan.Am J Kidney Dis. 2013 Jun;61(6):923-9. doi: 10.1053/j.ajkd.2012.12.028. Epub 2013 Feb 20. Am J Kidney Dis. 2013. PMID: 23433467
-
Kidney Stones After Bariatric Surgery: Risk Assessment and Mitigation.Bariatr Surg Pract Patient Care. 2017 Mar 1;12(1):3-9. doi: 10.1089/bari.2016.0048. Bariatr Surg Pract Patient Care. 2017. PMID: 28465866 Free PMC article. Review.
Cited by
-
Abdominal Obesity, Adipokines and Non-communicable Diseases.J Steroid Biochem Mol Biol. 2020 Oct;203:105737. doi: 10.1016/j.jsbmb.2020.105737. Epub 2020 Aug 18. J Steroid Biochem Mol Biol. 2020. PMID: 32818561 Free PMC article. Review.
-
Higher weight-adjusted waist index is associated with increased likelihood of kidney stones.Front Endocrinol (Lausanne). 2023 Sep 20;14:1234440. doi: 10.3389/fendo.2023.1234440. eCollection 2023. Front Endocrinol (Lausanne). 2023. PMID: 37800142 Free PMC article.
-
Effect of theobromine on dissolution of uric acid kidney stones.World J Urol. 2022 Aug;40(8):2105-2111. doi: 10.1007/s00345-022-04059-3. Epub 2022 Jun 11. World J Urol. 2022. PMID: 35689678 Free PMC article.
-
Association between cardiometabolic index and kidney stone from NHANES: a population-based study.Front Endocrinol (Lausanne). 2024 Oct 9;15:1408781. doi: 10.3389/fendo.2024.1408781. eCollection 2024. Front Endocrinol (Lausanne). 2024. PMID: 39444452 Free PMC article.
-
RIRS with FV-UAS vs. ESWL for the management of 1-2 cm lower pole renal calculi in obese patients: a prospective study.Front Med (Lausanne). 2024 Oct 30;11:1464491. doi: 10.3389/fmed.2024.1464491. eCollection 2024. Front Med (Lausanne). 2024. PMID: 39540048 Free PMC article.
References
-
- DeMaria E.J. Bariatric surgery for morbid obesity. N Engl J Med. 2007;356:2176–2183. - PubMed
-
- James W.P.T., Van de Werf F. Obesity management: the cardiovascular benefits. Eur Heart J. 2005;7(Suppl. L):L3–L4.
-
- Flum D.R., Khan T.V., Dellinger E.P. Toward the rational and equitable use of bariatric surgery. JAMA. 2007;298:1442. - PubMed
-
- Taylor E.N., Stampfer M.J., Curhan G.C. Obesity, weight gain, and the risk of kidney stones. JAMA. 2005;293:455–462. - PubMed
-
- Powell C.R., Stoller M.L., Schwartz B.F., Kane C., Gentle D.L., Bruce J.E. Impact of body weight on urinary electrolytes in urinary stone formers. Urology. 2000;55:825–830. - PubMed
Publication types
LinkOut - more resources
Full Text Sources
Research Materials