

Hepatorenal syndrome: Update on diagnosis and treatment
- PMID: 26558188
- PMCID: PMC4635371
- DOI: 10.5527/wjn.v4.i5.511
Hepatorenal syndrome: Update on diagnosis and treatment
Abstract
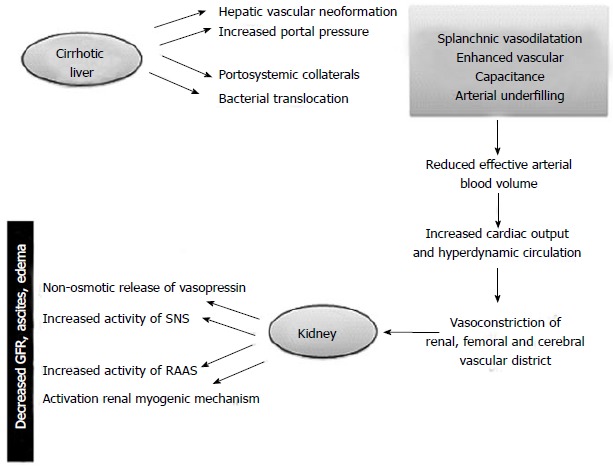
Acute kidney injury (AKI) is a common complication in patients with end-stage liver disease and advanced cirrhosis regardless of the underlying cause. Hepatorenal syndrome (HRS), a functional form of kidney failure, is one of the many possible causes of AKI. HRS is potentially reversible but involves highly complex pathogenetic mechanisms and equally complex clinical and therapeutic management. Once HRS has developed, it has a very poor prognosis. This review focuses on the diagnostic approach to HRS and discusses the therapeutic protocols currently adopted in clinical practice.
Keywords: Acute kidney injury; Cirrhosis; Diagnosis; Hepatorenal syndrome; Liver support system; Terlipressin; Treatment.
Figures
References
Publication types
LinkOut - more resources
Full Text Sources
Other Literature Sources
