

The 2015 European Thyroid Association Guidelines on Diagnosis and Treatment of Endogenous Subclinical Hyperthyroidism
- PMID: 26558232
- PMCID: PMC4637513
- DOI: 10.1159/000438750
The 2015 European Thyroid Association Guidelines on Diagnosis and Treatment of Endogenous Subclinical Hyperthyroidism
Abstract
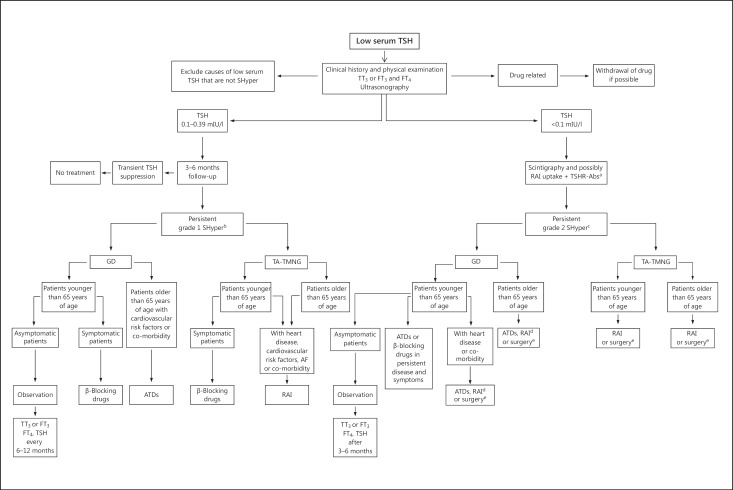
Endogenous subclinical hyperthyroidism (SHyper) is caused by Graves' disease, autonomously functioning thyroid nodules and multinodular goitre. Its diagnosis is based on a persistently subnormal serum thyroid-stimulating hormone (TSH) level with free thyroid hormone levels within their respective reference intervals. In 2014 the European Thyroid Association Executive Committee, given the controversies regarding the treatment of Endo SHyper, formed a task force to develop clinical practice guidelines based on the principles of evidence-based medicine. The task force recognized that recent meta-analyses, including those based on large prospective cohort studies, indicate that SHyper is associated with increased risk of coronary heart disease mortality, incident atrial fibrillation, heart failure, fractures and excess mortality in patients with serum TSH levels <0.1 mIU/l (grade 2 SHyper). Therefore, despite the absence of randomized prospective trials, there is evidence that treatment is indicated in patients older than 65 years with grade 2 SHyper to potentially avoid these serious cardiovascular events, fractures and the risk of progression to overt hyperthyroidism. Treatment could be considered in patients older than 65 years with TSH levels 0.1-0.39 mIU/l (grade 1 SHyper) because of their increased risk of atrial fibrillation, and might also be reasonable in younger (<65 years) symptomatic patients with grade 2 SHyper because of the risk of progression, especially in the presence of symptoms and/or underlying risk factors or co-morbidity. Finally, the task force concluded that there are no data to support treating SHyper in younger asymptomatic patients with grade 1 SHyper. These patients should be followed without treatment due to the low risk of progression to overt hyperthyroidism and the weaker evidence for adverse health outcomes.
Keywords: Antithyroid drugs; Bone risk; Cardiovascular risk; Cognition; Management; Progression; Radioactive iodine; Subclinical hyperthyroidism; Surgery.
Figures
References
-
- Surks MI, Ortiz E, Daniels GH, et al. Subclinical thyroid disease: scientific review and guidelines for diagnosis and management. JAMA. 2004;291:228–238. - PubMed
-
- Biondi B, Palmieri EA, Klain M, Schlumberger M, Filetti S, Lombardi G. Subclinical hyperthyroidism: clinical features and treatment options. Eur J Endocrinol. 2005;152:1–9. - PubMed
-
- Biondi B, Cooper DS. The clinical significance of subclinical thyroid dysfunction. Endocr Rev. 2008;29:76–131. - PubMed
-
- Bahn RS, Burch HB, Cooper DS, et al. Hyperthyroidism and other causes of thyrotoxicosis: management guidelines of the American Thyroid Association and American Association of Clinical Endocrinologists. Thyroid. 2011;21:593–646. - PubMed
-
- Cooper DS, Biondi B. Subclinical thyroid disease. Lancet. 2012;379:1142–1154. - PubMed
LinkOut - more resources
Full Text Sources
Other Literature Sources
