

Non-Adrenergic Vasopressors in Patients with or at Risk for Vasodilatory Shock. A Systematic Review and Meta-Analysis of Randomized Trials
- PMID: 26558621
- PMCID: PMC4641698
- DOI: 10.1371/journal.pone.0142605
Non-Adrenergic Vasopressors in Patients with or at Risk for Vasodilatory Shock. A Systematic Review and Meta-Analysis of Randomized Trials
Abstract
Introduction: Hypotensive state is frequently observed in several critical conditions. If an adequate mean arterial pressure is not promptly restored, insufficient tissue perfusion and organ dysfunction may develop. Fluids and catecholamines are the cornerstone of critical hypotensive states management. Catecholamines side effects such as increased myocardial oxygen consumption and development of arrhythmias are well known. Thus, in recent years, interest in catecholamine-sparing agents such as vasopressin, terlipressin and methylene blue has increased; however, few randomized trials, mostly with small sample sizes, have been performed. We therefore conducted a meta-analysis of randomized trials to investigate the effect of non-catecholaminergic vasopressors on mortality.
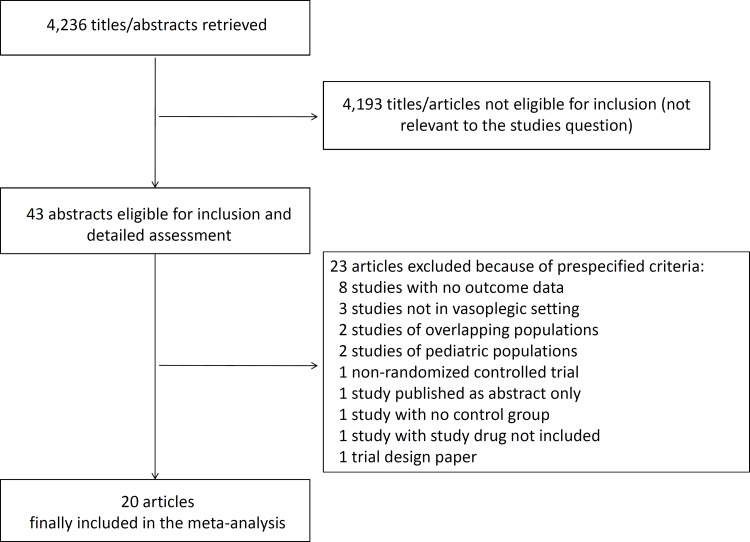
Methods: PubMed, BioMed Central and Embase were searched (update December 31st, 2014) by two independent investigators. Inclusion criteria were: random allocation to treatment, at least one group receiving a non-catecholaminergic vasopressor, patients with or at risk for vasodilatory shock. Exclusion criteria were: crossover studies, pediatric population, non-human studies, studies published as abstract only, lack of data on mortality. Studied drugs were vasopressin, terlipressin and methylene blue. Primary endpoint was mortality at the longest follow-up available.
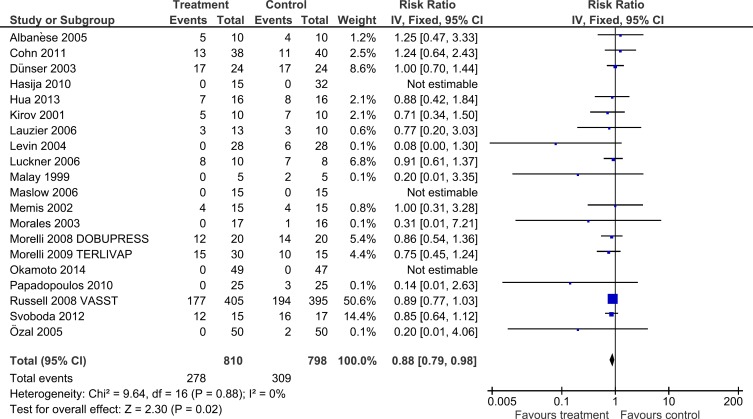
Results: A total of 1,608 patients from 20 studies were included in our analysis. The studied settings were sepsis (10/20 studies [50%]), cardiac surgery (7/20 [35%]), vasodilatory shock due to any cause (2/20 [19%]), and acute traumatic injury (1/20 [5%]). Overall, pooled estimates showed that treatment with non-catecholaminergic agents improves survival (278/810 [34.3%] versus 309/798 [38.7%], risk ratio = 0.88, 95% confidence interval = 0.79 to 0.98, p = 0.02). None of the drugs was associated with significant reduction in mortality when analyzed independently. Results were not confirmed when analyzing studies with a low risk of bias.
Conclusions: Catecholamine-sparing agents in patients with or at risk for vasodilatory shock may improve survival. Further researches on this topic are needed to confirm the finding.
Conflict of interest statement
Figures
References
-
- Bourgoin A, Leone M, Delmas A, Garnier F, Albanèse J, Martin C. Increasing mean arterial pressure in patients with septic shock: effects on oxygen variables and renal function. Crit Care Med. 2005;33: 780–6. - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
