

Performance of C-reactive protein and procalcitonin to distinguish viral from bacterial and malarial causes of fever in Southeast Asia
- PMID: 26558692
- PMCID: PMC4642613
- DOI: 10.1186/s12879-015-1272-6
Performance of C-reactive protein and procalcitonin to distinguish viral from bacterial and malarial causes of fever in Southeast Asia
Abstract
Background: Poor targeting of antimicrobial drugs contributes to the millions of deaths each year from malaria, pneumonia, and other tropical infectious diseases. While malaria rapid diagnostic tests have improved use of antimalarial drugs, there are no similar tests to guide the use of antibiotics in undifferentiated fevers. In this study we estimate the diagnostic accuracy of two well established biomarkers of bacterial infection, procalcitonin and C-reactive protein (CRP) in discriminating between common viral and bacterial infections in malaria endemic settings of Southeast Asia.
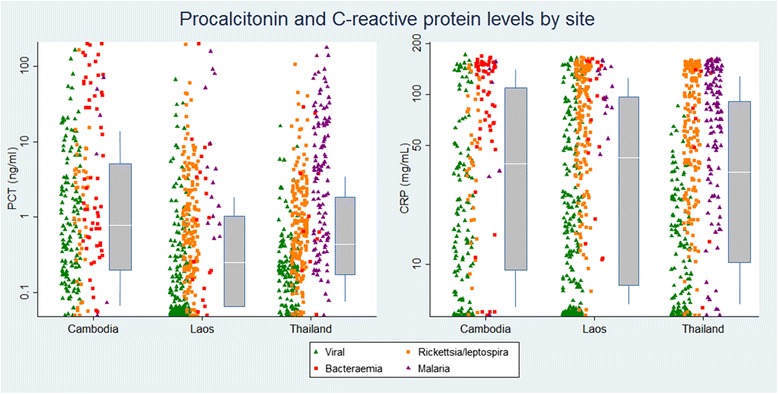
Methods: Serum procalcitonin and CRP levels were measured in stored serum samples from febrile patients enrolled in three prospective studies conducted in Cambodia, Laos and, Thailand. Of the 1372 patients with a microbiologically confirmed diagnosis, 1105 had a single viral, bacterial or malarial infection. Procalcitonin and CRP levels were compared amongst these aetiological groups and their sensitivity and specificity in distinguishing bacterial infections and bacteraemias from viral infections were estimated using standard thresholds.
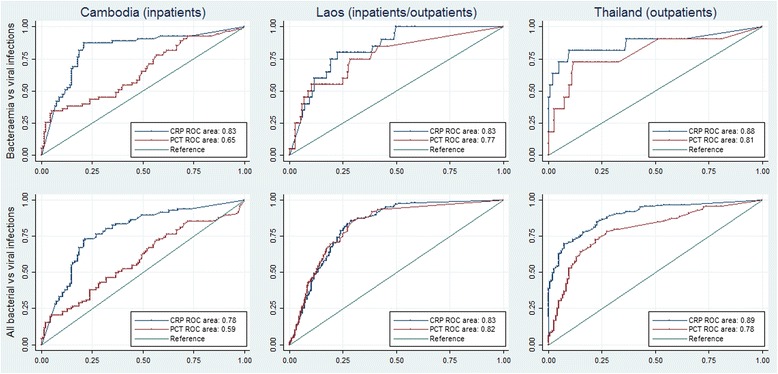
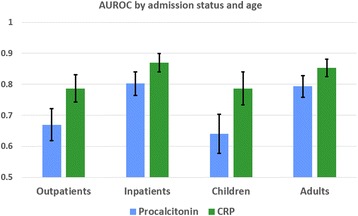
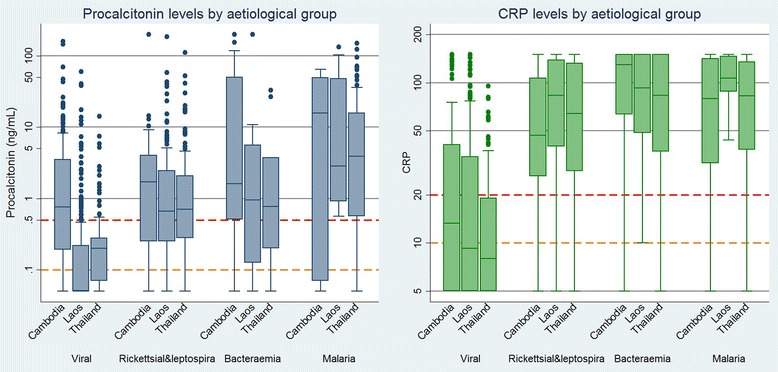
Results: Serum concentrations of both biomarkers were significantly higher in bacterial infections and malaria than in viral infections. The AUROC for CRP in discriminating between bacterial and viral infections was 0.83 (0.81-0.86) compared with 0.74 (0.71-0.77) for procalcitonin (p < 0.0001). This relative advantage was evident in all sites and when stratifying patients by age and admission status. For CRP at a threshold of 10 mg/L, the sensitivity of detecting bacterial infections was 95% with a specificity of 49%. At a threshold of 20 mg/L sensitivity was 86% with a specificity of 67%. For procalcitonin at a low threshold of 0.1 ng/mL the sensitivity was 90% with a specificity of 39%. At a higher threshold of 0.5 ng/ul sensitivity was 60% with a specificity of 76%.
Conclusion: In samples from febrile patients with mono-infections from rural settings in Southeast Asia, CRP was a highly sensitive and moderately specific biomarker for discriminating between viral and bacterial infections. Use of a CRP rapid test in peripheral health settings could potentially be a simple and affordable measure to better identify patients in need of antibacterial treatment and part of a global strategy to combat the emergence of antibiotic resistance.
Figures
References
-
- Lozano R, Naghavi M, Foreman K, Lim S, Shibuya K, Aboyans V, et al. Global and regional mortality from 235 causes of death for 20 age groups in 1990 and 2010: a systematic analysis for the Global Burden of Disease Study 2010. Lancet. 2012;380(9859):2095–2128. doi: 10.1016/S0140-6736(12)61728-0. - DOI - PMC - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
Miscellaneous
