

A Retrospective Longitudinal Within-Subject Risk Interval Analysis of Immunoglobulin Treatment for Recurrent Acute Exacerbation of Chronic Obstructive Pulmonary Disease
- PMID: 26558756
- PMCID: PMC4641695
- DOI: 10.1371/journal.pone.0142205
A Retrospective Longitudinal Within-Subject Risk Interval Analysis of Immunoglobulin Treatment for Recurrent Acute Exacerbation of Chronic Obstructive Pulmonary Disease
Abstract
Background: Recurrent acute exacerbations of chronic obstructive pulmonary disease (AECOPD) are common, debilitating, costly and often difficult to prevent.
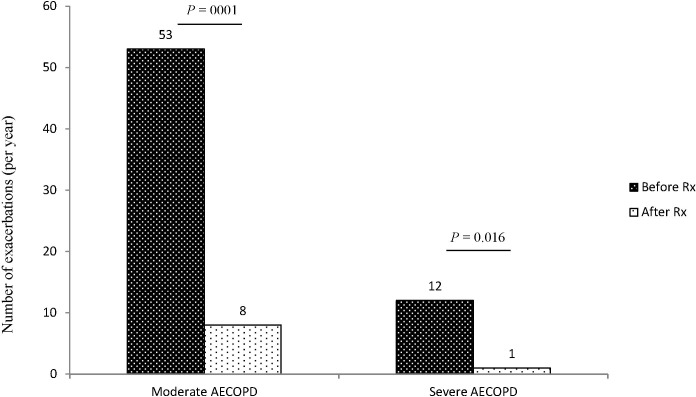
Methods: We reviewed records of patients who had COPD and immunoglobulin (Ig) treatment as adjunctive preventative treatment for AECOPD, and documented all AECOPD episodes for one year before and after initiation of Ig treatment. We graded AECOPD episodes as moderate for prescription of antibiotics and/or corticosteroids or for visit to the Emergency Department, and as severe for hospital admission. We conducted a retrospective within-subject self-controlled risk interval analysis to compare the outcome of annual AECOPD rate before and after treatment.
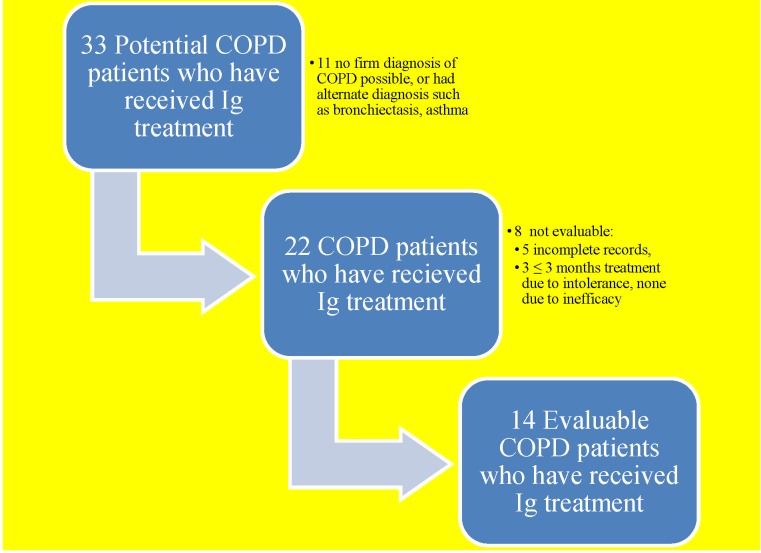
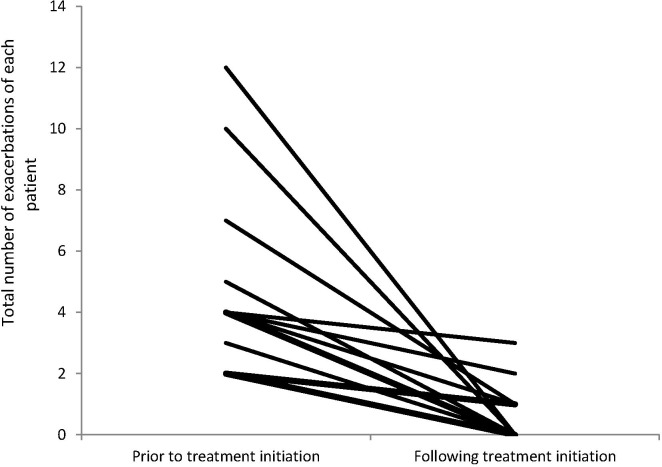
Results: We identified 22 cases of certain COPD, of which three had early discontinuation of Ig treatment due to rash and local swelling to subcutaneous Ig, and five had incomplete records leaving 14 cases for analyses. The median baseline IgG level was 5.9 g/L (interquartile range 4.1-7.4). Eight had CT radiographic bronchiectasis. Overall, the incidence of AECOPD was consistently and significantly reduced in frequency from mean 4.7 (± 3.1) per patient-year before, to 0.6 (± 1.0) after the Ig treatment (p = 0.0001). There were twelve episodes of severe AECOPD (in seven cases) in the year prior, and one in the year after Ig treatment initiation (p = 0.016).
Conclusions: Ig treatment appears to decrease the frequency of moderate and severe recurrent AECOPD. A prospective, controlled evaluation of adjunctive Ig treatment to standard therapy of recurrent AECOPD is warranted.
Conflict of interest statement
Figures
Similar articles
-
Corticosteroids in the treatment of acute exacerbations of chronic obstructive pulmonary disease.Int J Chron Obstruct Pulmon Dis. 2014 May 3;9:421-30. doi: 10.2147/COPD.S51012. eCollection 2014. Int J Chron Obstruct Pulmon Dis. 2014. PMID: 24833897 Free PMC article. Review.
-
Microorganisms resistant to conventional antimicrobials in acute exacerbations of chronic obstructive pulmonary disease.Respir Res. 2018 Jun 15;19(1):119. doi: 10.1186/s12931-018-0820-1. Respir Res. 2018. PMID: 29907113 Free PMC article.
-
Exacerbation recovery patterns in newly diagnosed or maintenance treatment-naïve patients with COPD: secondary analyses of TICARI 1 trial data.Int J Chron Obstruct Pulmon Dis. 2018 May 10;13:1515-1525. doi: 10.2147/COPD.S149669. eCollection 2018. Int J Chron Obstruct Pulmon Dis. 2018. PMID: 29785101 Free PMC article. Clinical Trial.
-
Self-report underestimates the frequency of the acute respiratory exacerbations of COPD but is associated with BAL neutrophilia and lymphocytosis: an observational study.BMC Pulm Med. 2024 Sep 2;24(1):433. doi: 10.1186/s12890-024-03239-8. BMC Pulm Med. 2024. PMID: 39223571 Free PMC article.
-
Polyvalent Immunoglobulin as a Potential Treatment Option for Patients with Recurrent COPD Exacerbations.Int J Chron Obstruct Pulmon Dis. 2021 Mar 2;16:545-552. doi: 10.2147/COPD.S283832. eCollection 2021. Int J Chron Obstruct Pulmon Dis. 2021. PMID: 33688179 Free PMC article. Review.
Cited by
-
The impact of IgG subclass deficiency on the risk of mortality in hospitalized patients with COPD.Respir Res. 2022 May 31;23(1):141. doi: 10.1186/s12931-022-02052-3. Respir Res. 2022. PMID: 35641962 Free PMC article.
-
Respiratory infectious burden in a cohort of antibody deficiency patients treated with immunoglobulin replacement therapy: The impact of lung pathology and gastroesophageal reflux disease.J Allergy Clin Immunol Glob. 2023 Jul 1;2(4):100133. doi: 10.1016/j.jacig.2023.100133. eCollection 2023 Nov. J Allergy Clin Immunol Glob. 2023. PMID: 37781665 Free PMC article.
-
Study protocol: a randomized, double-blind, parallel, two-arm, placebo control trial investigating the feasibility and safety of immunoglobulin treatment in COPD patients for prevention of frequent recurrent exacerbations.Pilot Feasibility Stud. 2018 Aug 11;4:135. doi: 10.1186/s40814-018-0327-z. eCollection 2018. Pilot Feasibility Stud. 2018. PMID: 30116551 Free PMC article.
-
Lower serum IgA is associated with COPD exacerbation risk in SPIROMICS.PLoS One. 2018 Apr 12;13(4):e0194924. doi: 10.1371/journal.pone.0194924. eCollection 2018. PLoS One. 2018. PMID: 29649230 Free PMC article.
-
Effectiveness of immunoglobulin replacement therapy in preventing infections in patients with chronic obstructive pulmonary disease: a systematic review.Allergy Asthma Clin Immunol. 2024 Apr 10;20(1):30. doi: 10.1186/s13223-024-00886-8. Allergy Asthma Clin Immunol. 2024. PMID: 38600554 Free PMC article.
References
-
- Hoyert DL, Xu J. Deaths: preliminary data for 2011. Natl Vital Stat Rep 2012. October 10;61(6):1–51. - PubMed
-
- Seemungal TA, Donaldson GC, Paul EA, Bestall JC, Jeffries DJ, Wedzicha JA. Effect of exacerbation on quality of life in patients with chronic obstructive pulmonary disease. Am J Respir Crit Care Med 1998. May;157(5 Pt 1):1418–1422. - PubMed
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
