

A Revised Classification System and Recommendations From the Baltimore Consensus Meeting for Neoplastic Precursor Lesions in the Pancreas
- PMID: 26559377
- PMCID: PMC4646710
- DOI: 10.1097/PAS.0000000000000533
A Revised Classification System and Recommendations From the Baltimore Consensus Meeting for Neoplastic Precursor Lesions in the Pancreas
Abstract
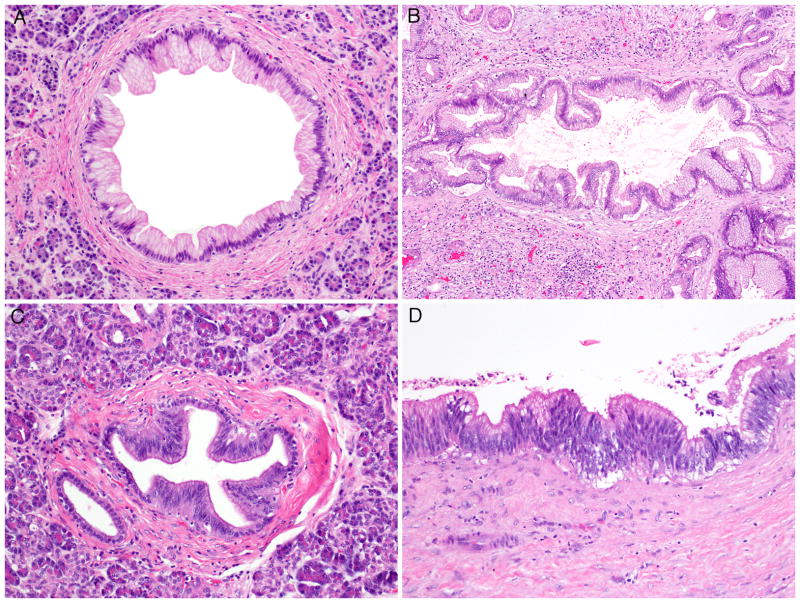
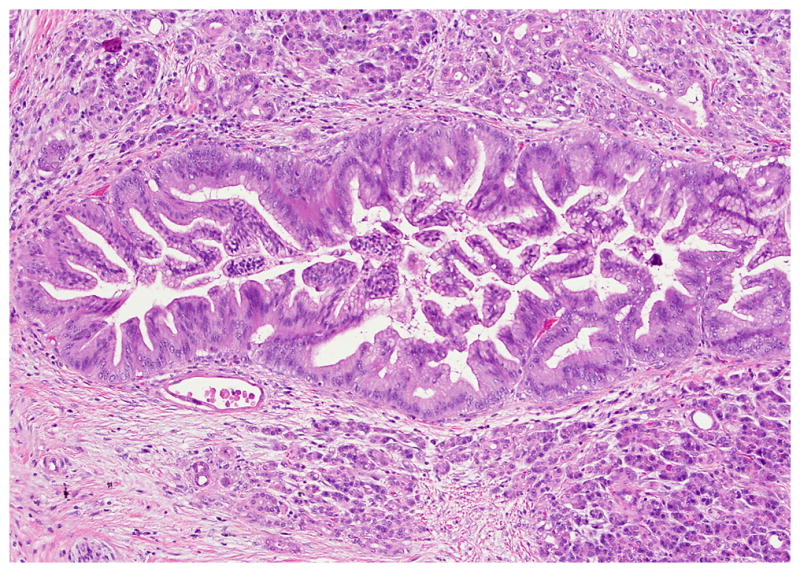
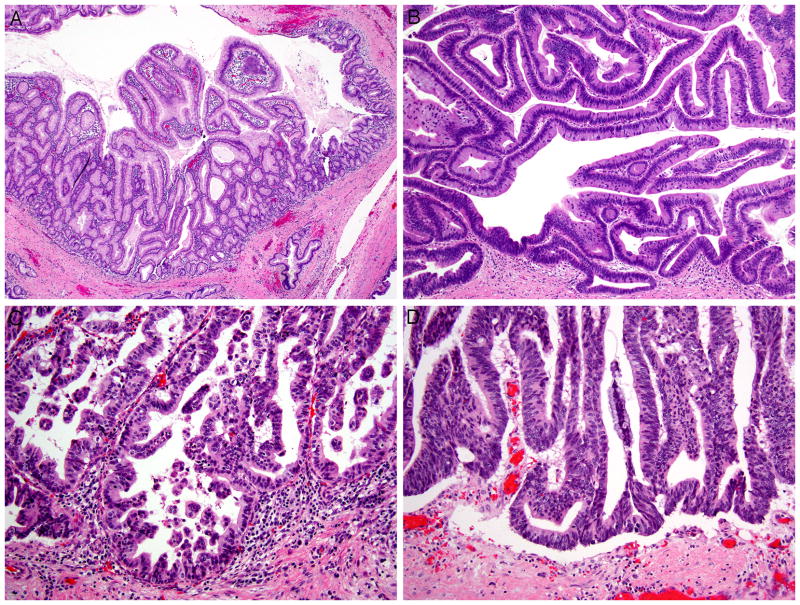
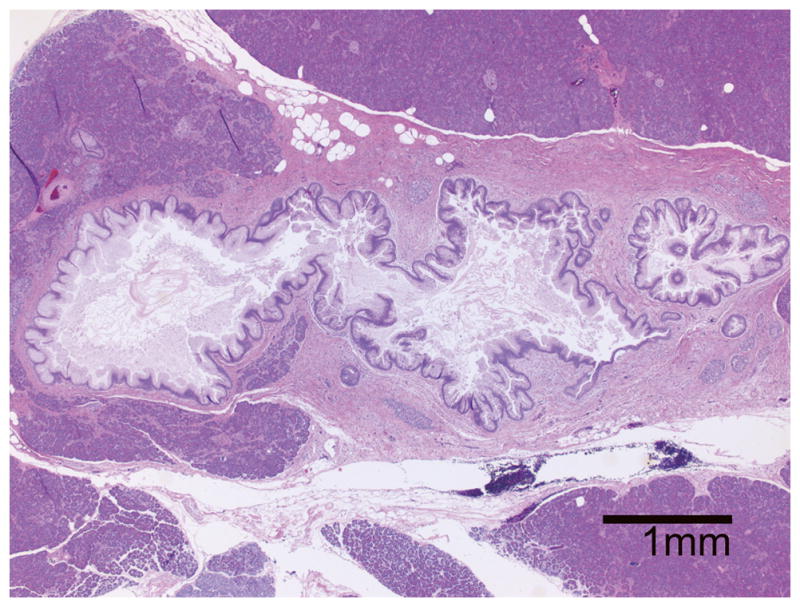
International experts met to discuss recent advances and to revise the 2004 recommendations for assessing and reporting precursor lesions to invasive carcinomas of the pancreas, including pancreatic intraepithelial neoplasia (PanIN), intraductal papillary mucinous neoplasm (IPMN), mucinous cystic neoplasm, and other lesions. Consensus recommendations include the following: (1) To improve concordance and to align with practical consequences, a 2-tiered system (low vs. high grade) is proposed for all precursor lesions, with the provision that the current PanIN-2 and neoplasms with intermediate-grade dysplasia now be categorized as low grade. Thus, "high-grade dysplasia" is to be reserved for only the uppermost end of the spectrum ("carcinoma in situ"-type lesions). (2) Current data indicate that PanIN of any grade at a margin of a resected pancreas with invasive carcinoma does not have prognostic implications; the clinical significance of dysplasia at a margin in a resected pancreas with IPMN lacking invasive carcinoma remains to be determined. (3) Intraductal lesions 0.5 to 1 cm can be either large PanINs or small IPMNs. The term "incipient IPMN" should be reserved for lesions in this size with intestinal or oncocytic papillae or GNAS mutations. (4) Measurement of the distance between an IPMN and invasive carcinoma and sampling of intervening tissue are recommended to assess concomitant versus associated status. Conceptually, concomitant invasive carcinoma (in contrast with the "associated" group) ought to be genetically distinct from an IPMN elsewhere in the gland. (5) "Intraductal spread of invasive carcinoma" (aka, "colonization") is recommended to describe lesions of invasive carcinoma invading back into and extending along the ductal system, which may morphologically mimic high-grade PanIN or even IPMN. (6) "Simple mucinous cyst" is recommended to describe cysts >1 cm having gastric-type flat mucinous lining at most minimal atypia without ovarian-type stroma to distinguish them from IPMN. (7) Human lesions resembling the acinar to ductal metaplasia and atypical flat lesions of genetically engineered mouse models exist and may reflect an alternate pathway of carcinogenesis; however, their biological significance requires further study. These revised recommendations are expected to improve our management and understanding of precursor lesions in the pancreas.
Conflict of interest statement
Figures
References
-
- Hruban RH, Adsay NV, Albores-Saavedra J, et al. Pancreatic intraepithelial neoplasia: a new nomenclature and classification system for pancreatic duct lesions. Am J Surg Pathol. 2001;25:579–586. - PubMed
-
- Hruban RH, Takaori K, Klimstra DS, et al. An illustrated consensus on the classification of pancreatic intraepithelial neoplasia and intraductal papillary mucinous neoplasms. Am J Surg Pathol. 2004;28:977–987. - PubMed
-
- Hruban RH, Pitman MB, Klimstra DS. Tumors of the pancreas. Washington, DC: American Registry of Pathology; 2007.
-
- Adsay NV, Fukushima N, Furukawa T, et al. Intraductal neoplasms of the pancreas. In: Bosman FT, Hruban RH, Carneiro F, et al., editors. WHO Classification of Tumours of the Digestive System. Lyon: IARC; 2010. pp. 304–313.
-
- Hruban RH, Adsay NV, Albores-Saavedra J, et al. Pathology of genetically engineered mouse models of pancreatic exocrine cancer: consensus report and recommendations. Cancer Res. 2006;66:95–106. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Miscellaneous
