

Development and validation of risk prediction equations to estimate future risk of blindness and lower limb amputation in patients with diabetes: cohort study
- PMID: 26560308
- PMCID: PMC4641884
- DOI: 10.1136/bmj.h5441
Development and validation of risk prediction equations to estimate future risk of blindness and lower limb amputation in patients with diabetes: cohort study
Abstract
Study question: Is it possible to develop and externally validate risk prediction equations to estimate the 10 year risk of blindness and lower limb amputation in patients with diabetes aged 25-84 years?
Methods: This was a prospective cohort study using routinely collected data from general practices in England contributing to the QResearch and Clinical Practice Research Datalink (CPRD) databases during the study period 1998-2014. The equations were developed using 763 QResearch practices (n=454,575 patients with diabetes) and validated in 254 different QResearch practices (n=142,419) and 357 CPRD practices (n=206,050). Cox proportional hazards models were used to derive separate risk equations for blindness and amputation in men and women that could be evaluated at 10 years. Measures of calibration and discrimination were calculated in the two validation cohorts.
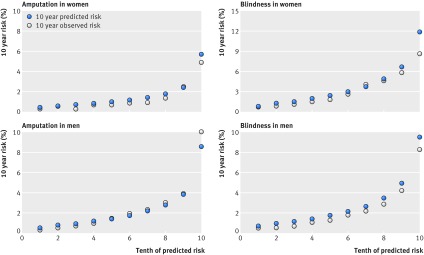
Study answer and limitations: Risk prediction equations to quantify absolute risk of blindness and amputation in men and women with diabetes have been developed and externally validated. In the QResearch derivation cohort, 4822 new cases of lower limb amputation and 8063 new cases of blindness occurred during follow-up. The risk equations were well calibrated in both validation cohorts. Discrimination was good in men in the external CPRD cohort for amputation (D statistic 1.69, Harrell's C statistic 0.77) and blindness (D statistic 1.40, Harrell's C statistic 0.73), with similar results in women and in the QResearch validation cohort. The algorithms are based on variables that patients are likely to know or that are routinely recorded in general practice computer systems. They can be used to identify patients at high risk for prevention or further assessment. Limitations include lack of formally adjudicated outcomes, information bias, and missing data.
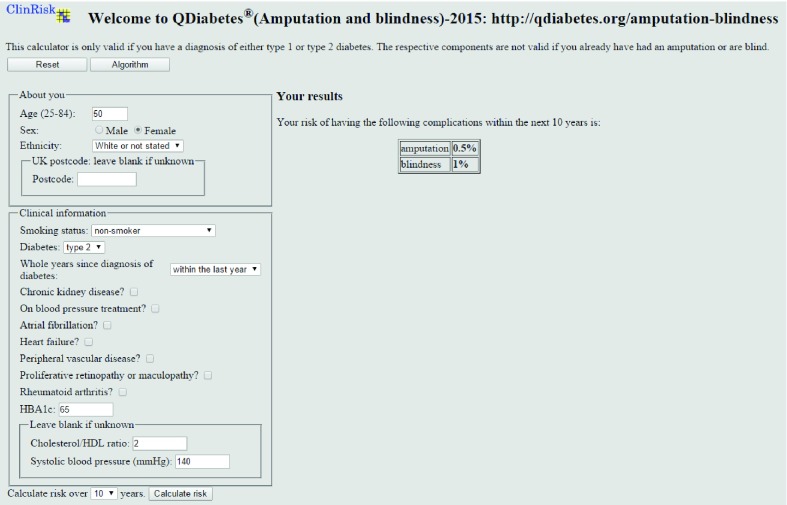
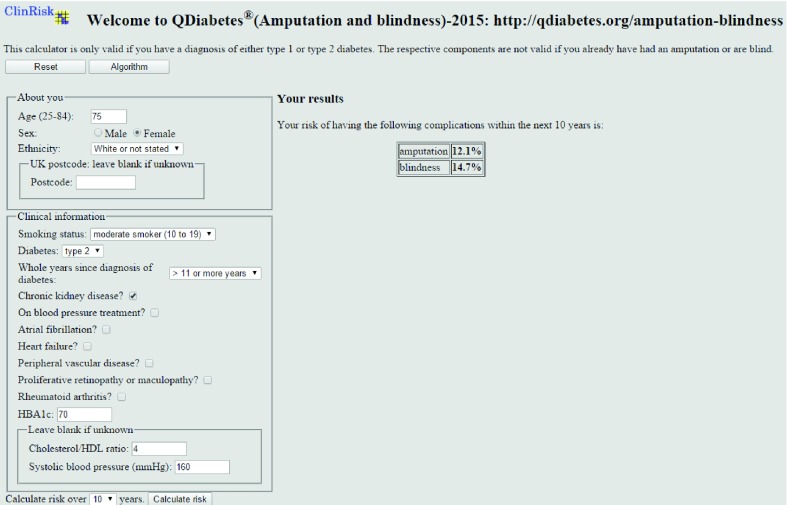
What this study adds: Patients with type 1 or type 2 diabetes are at increased risk of blindness and amputation but generally do not have accurate assessments of the magnitude of their individual risks. The new algorithms calculate the absolute risk of developing these complications over a 10 year period in patients with diabetes, taking account of their individual risk factors.
Funding, competing interests, data sharing: JH-C is co-director of QResearch, a not for profit organisation which is a joint partnership between the University of Nottingham and Egton Medical Information Systems, and is also a paid director of ClinRisk Ltd. CC is a paid consultant statistician for ClinRisk Ltd.
© Hippisley-Cox et al 2015.
Conflict of interest statement
Competing interests: Both authors have completed the ICMJE uniform disclosure form at
Figures
Comment in
-
Identifying people with diabetes at high risk of blindness and amputation.BMJ. 2015 Nov 11;351:h5643. doi: 10.1136/bmj.h5643. BMJ. 2015. PMID: 26561339 No abstract available.
References
-
- Diabetes Control and Complications Trial Research Group. The effect of intensive treatment of diabetes on the development and progression of long-term complications in insulin-dependent diabetes mellitus. N Engl J Med 1993;329:977-86. - PubMed
-
- Health and Social Care Information Centre. National Diabetes Audit 2012-2013. Report 2: complications and mortality. HSCIC, 2014:37.
-
- UK Prospective Diabetes Study (UKPDS) Group. Intensive blood-glucose control with sulphonylureas or insulin compared with conventional treatment and risk of complications in patients with type 2 diabetes (UKPDS 33). Lancet 1998;352:837-53. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical