

Potential confounding in the association between short birth intervals and increased neonatal, infant, and child mortality
- PMID: 26562139
- PMCID: PMC4642358
- DOI: 10.3402/gha.v8.29724
Potential confounding in the association between short birth intervals and increased neonatal, infant, and child mortality
Abstract
Background: Recent steep declines in child mortality have been attributed in part to increased use of contraceptives and the resulting change in fertility behaviour, including an increase in the time between births. Previous observational studies have documented strong associations between short birth spacing and an increase in the risk of neonatal, infant, and under-five mortality, compared to births with longer preceding birth intervals. In this analysis, we compare two methods to estimate the association between short birth intervals and mortality risk to better inform modelling efforts linking family planning and mortality in children.
Objectives: Our goal was to estimate the mortality risk for neonates, infants, and young children by preceding birth space using household survey data, controlling for mother-level factors and to compare the results to those from previous analyses with survey data.
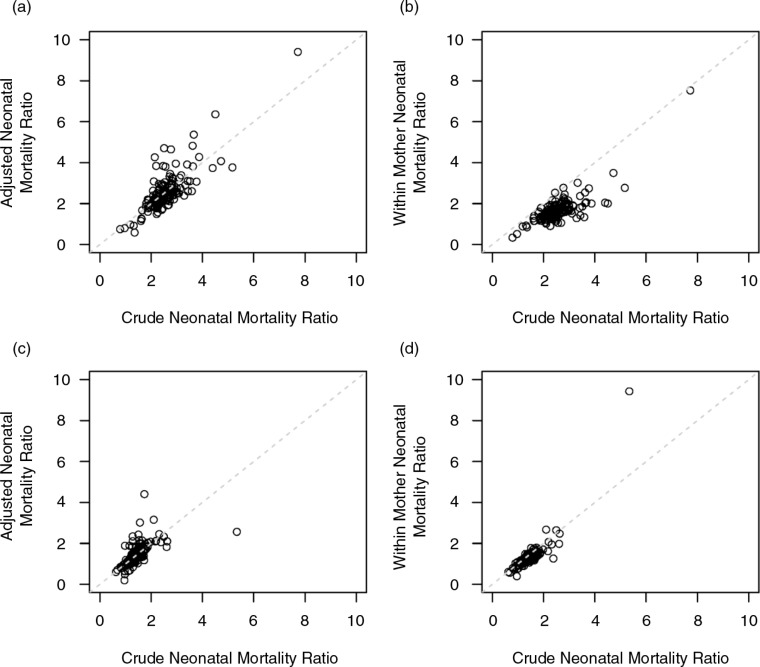
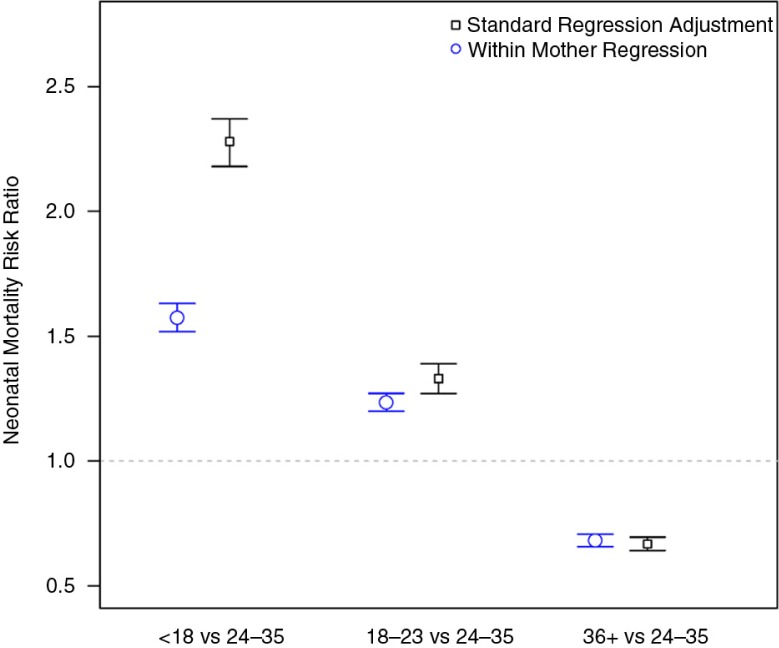
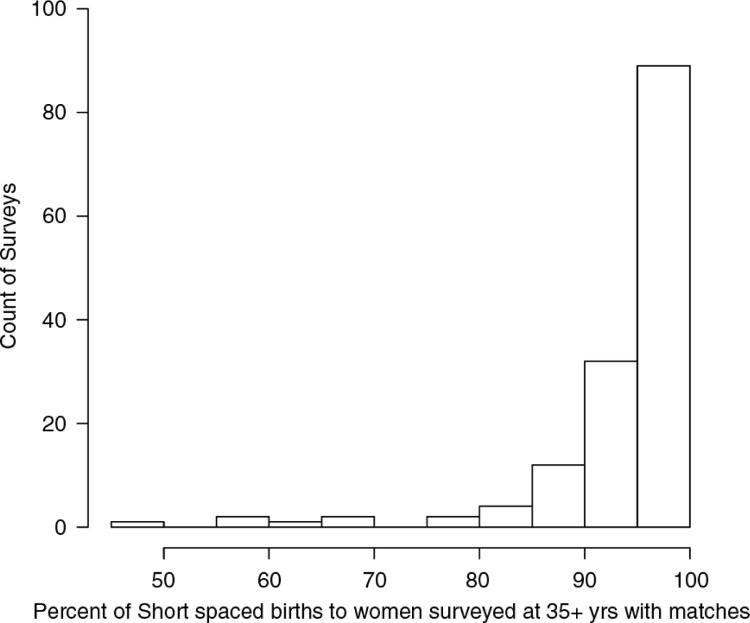
Design: We assessed the potential for confounding when estimating the relative mortality risk by preceding birth interval and estimated mortality risk by birth interval in four categories: less than 18 months, 18-23 months, 24-35 months, and 36 months or longer. We estimated the relative risks among women who were 35 and older at the time of the survey with two methods: in a Cox proportional hazards regression adjusting for potential confounders and also by stratifying Cox regression by mother, to control for all factors that remain constant over a woman's childbearing years. We estimated the overall effects for birth spacing in a meta-analysis with random survey effects.
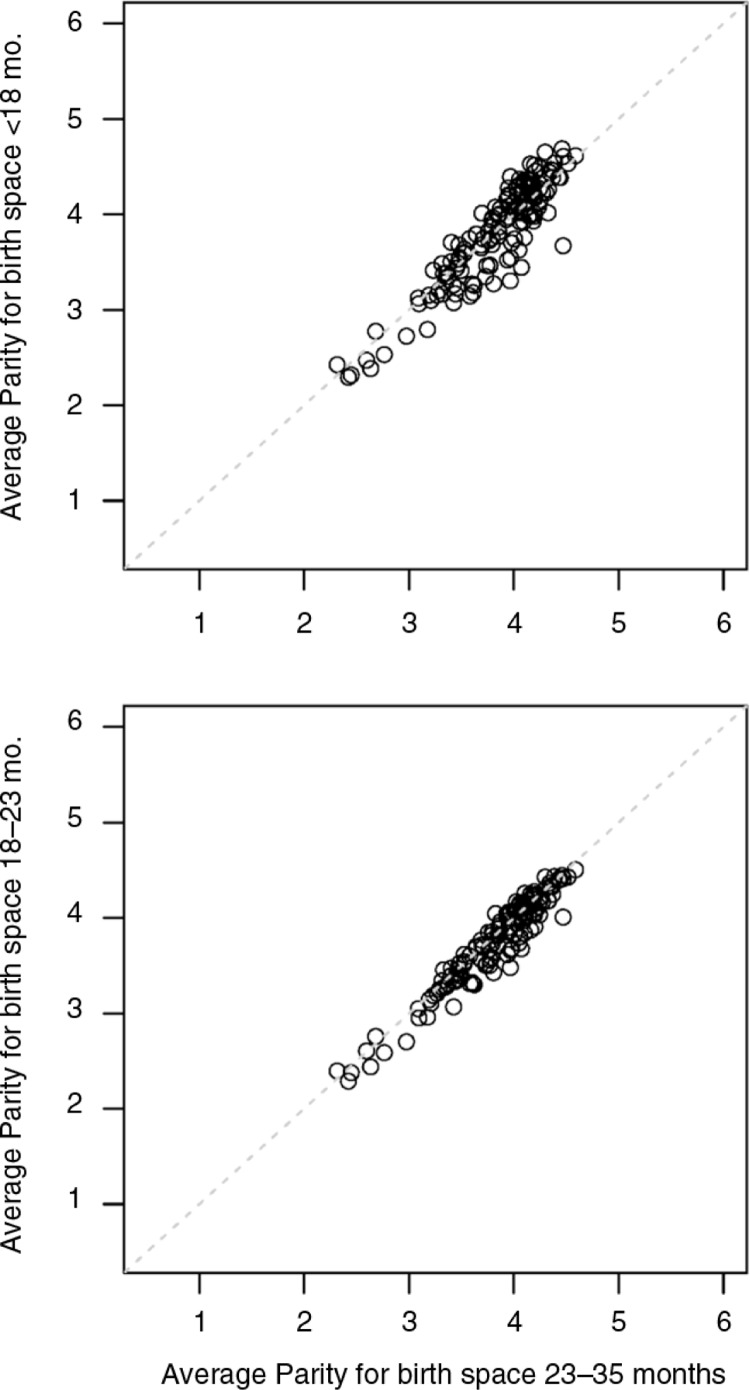
Results: We identified several factors known for their associations with neonatal, infant, and child mortality that are also associated with preceding birth interval. When estimating the effect of birth spacing on mortality, we found that regression adjustment for these factors does not substantially change the risk ratio for short birth intervals compared to an unadjusted mortality ratio. For birth intervals less than 18 months, standard regression adjustment for confounding factors estimated a risk ratio for neonatal mortality of 2.28 (95% confidence interval: 2.18-2.37). This same effect estimated within mother is 1.57 (95% confidence interval: 1.52-1.63), a decline of almost one-third in the effect on neonatal mortality.
Conclusions: Neonatal, infant, and child mortality are strongly and significantly related to preceding birth interval, where births within a short interval of time after the previous birth have increased mortality. Previous analyses have demonstrated this relationship on average across all births; however, women who have short spaces between births are different from women with long spaces. Among women 35 years and older where a comparison of birth spaces within mother is possible, we find a much reduced although still significant effect of short birth spaces on child mortality.
Keywords: attributable fraction; confounding; contraception rate; family planning; fertility.
Figures
References
-
- Winikoff B. The effects of birth spacing on child and maternal health. Stud Fam Plann. 1983;14:231–45. - PubMed
-
- Conde-Agudelo A, Rosas-Bermudez A, Kafury-Goeta A. Birth spacing and risk of adverse perinatal outcomes: a meta-analysis. JAMA. 2006;295:1809–23. - PubMed
-
- Arnold F. Assessment of the quality of birth history data in the demographic and health surveys. Report No. 1: an assessment of DHS-I data quality. 1990. Available from: http://dhsprogram.com/pubs/pdf/MR1/MR1.pdf [cited 27 July 2015].
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources