

Extracellular matrix remodeling in wound healing of critical size defects in the mitral valve leaflet
- PMID: 26563105
- PMCID: PMC10578972
- DOI: 10.1007/s00380-015-0768-8
Extracellular matrix remodeling in wound healing of critical size defects in the mitral valve leaflet
Abstract
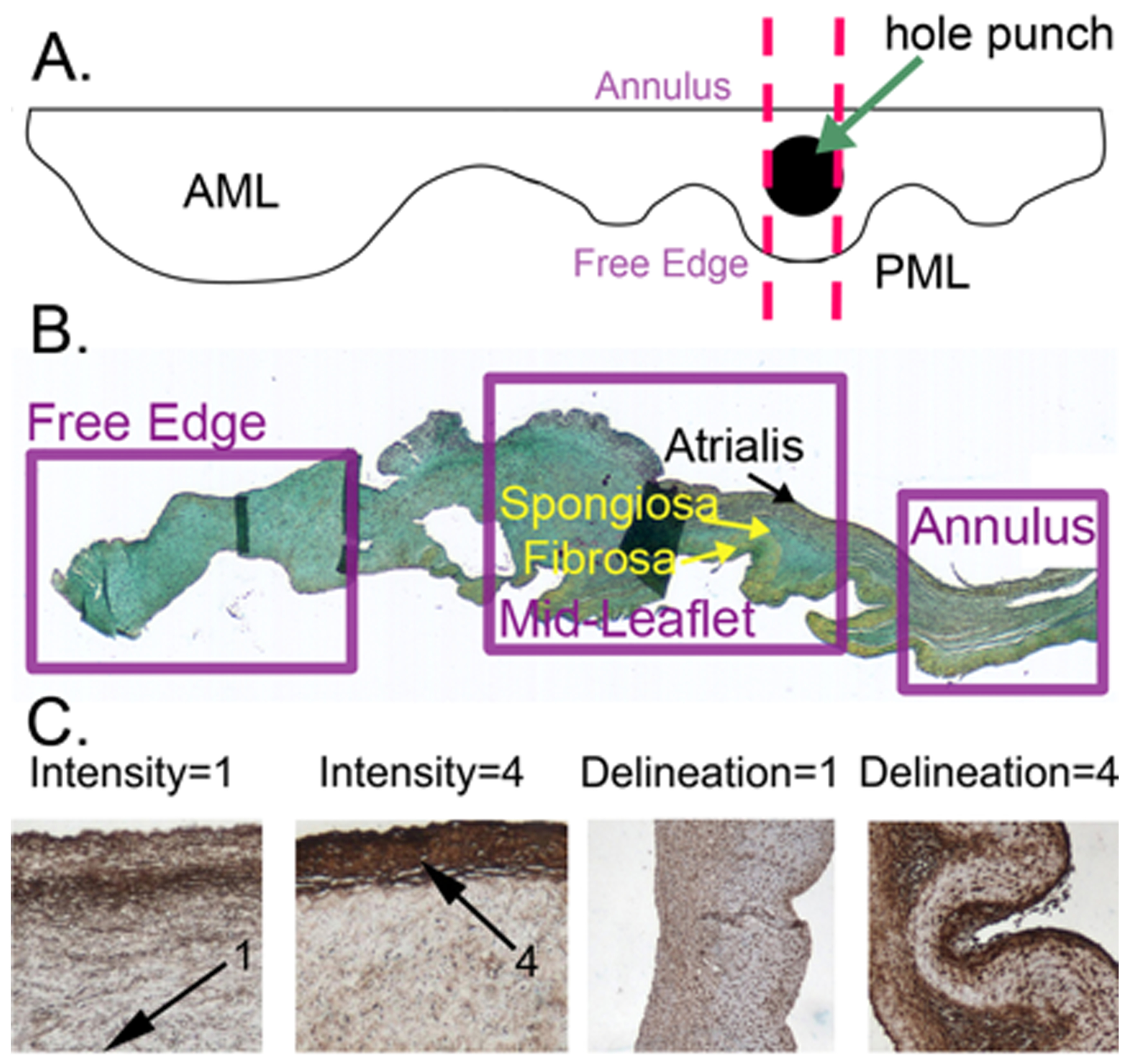
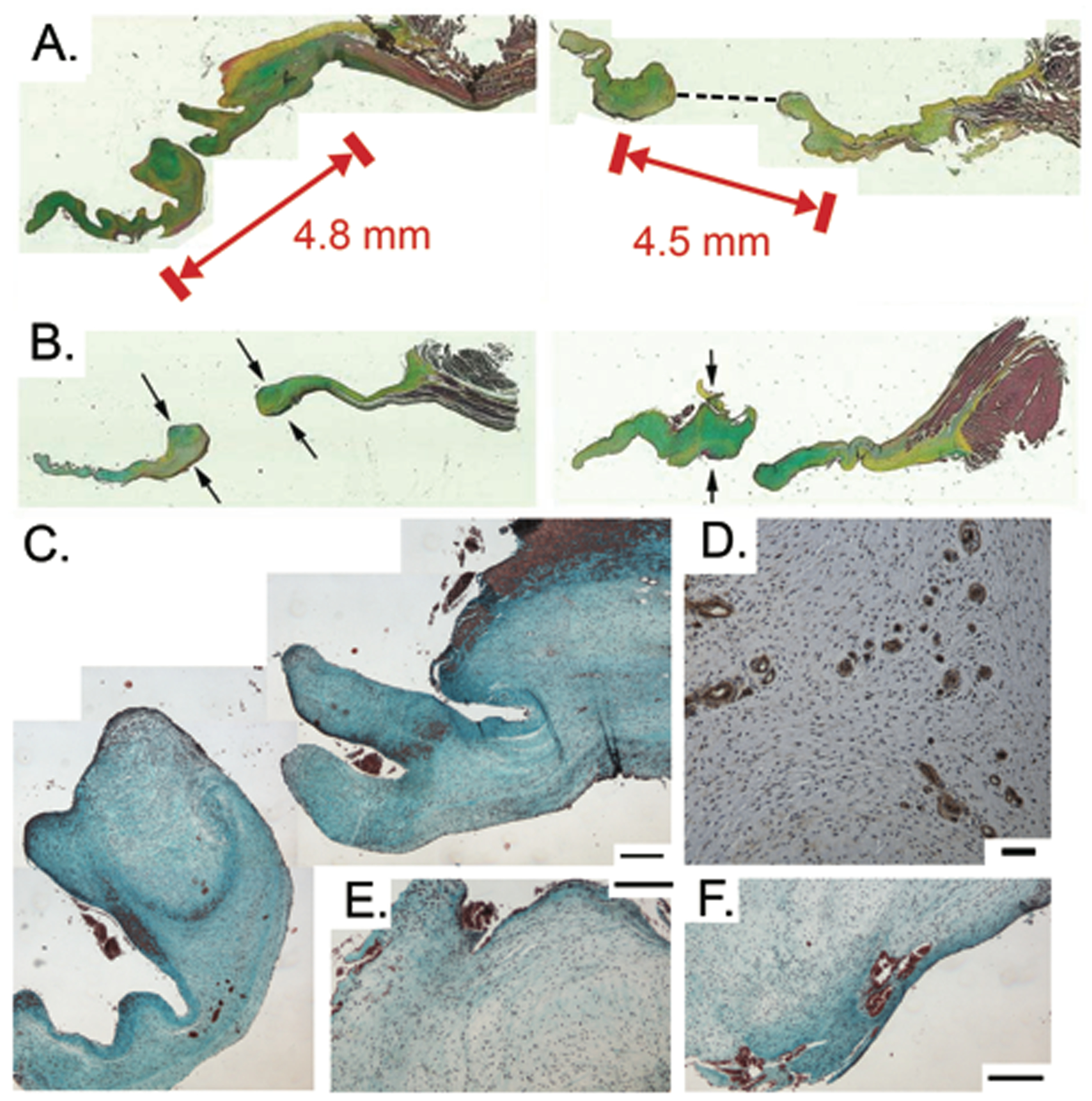
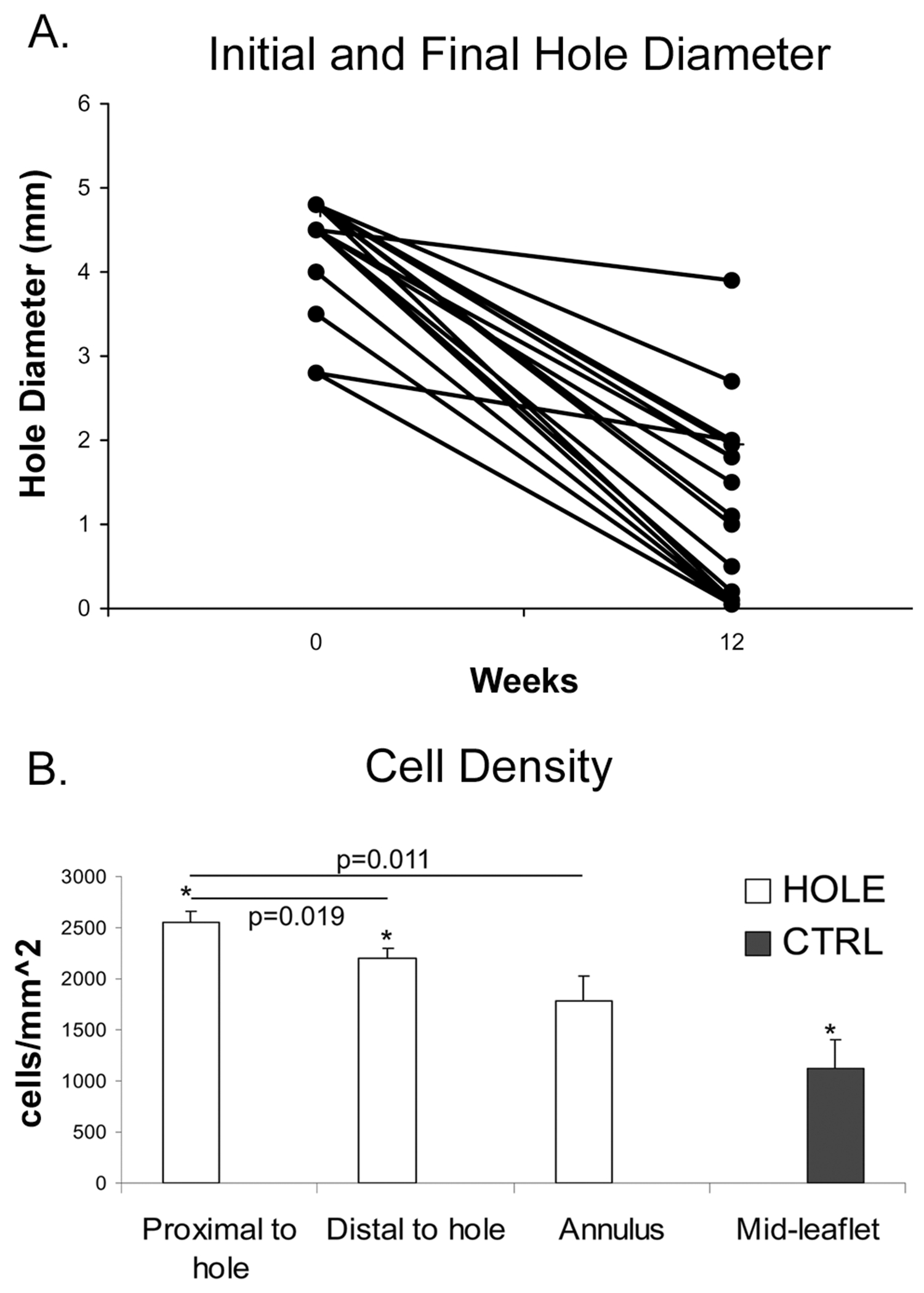
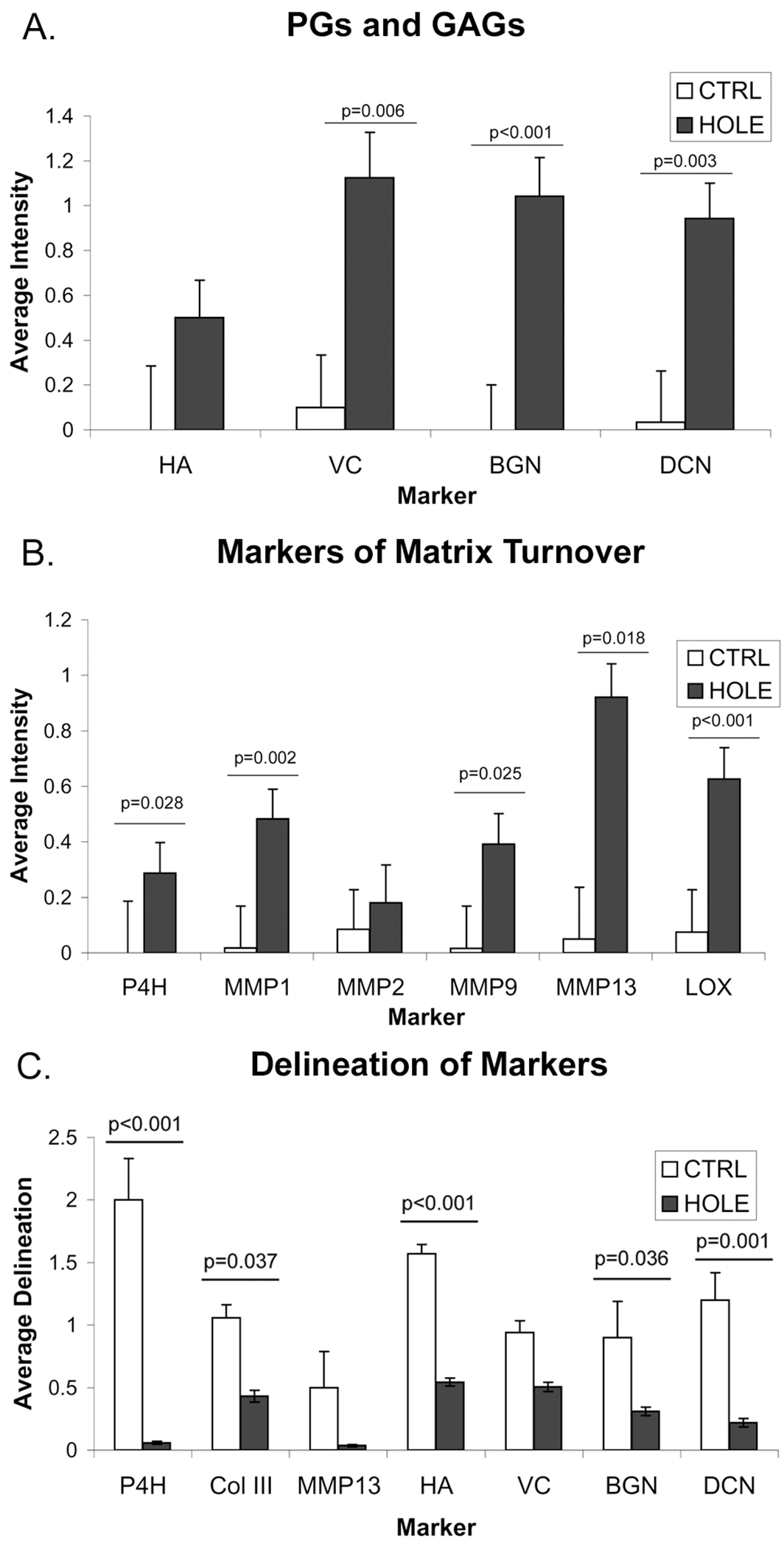
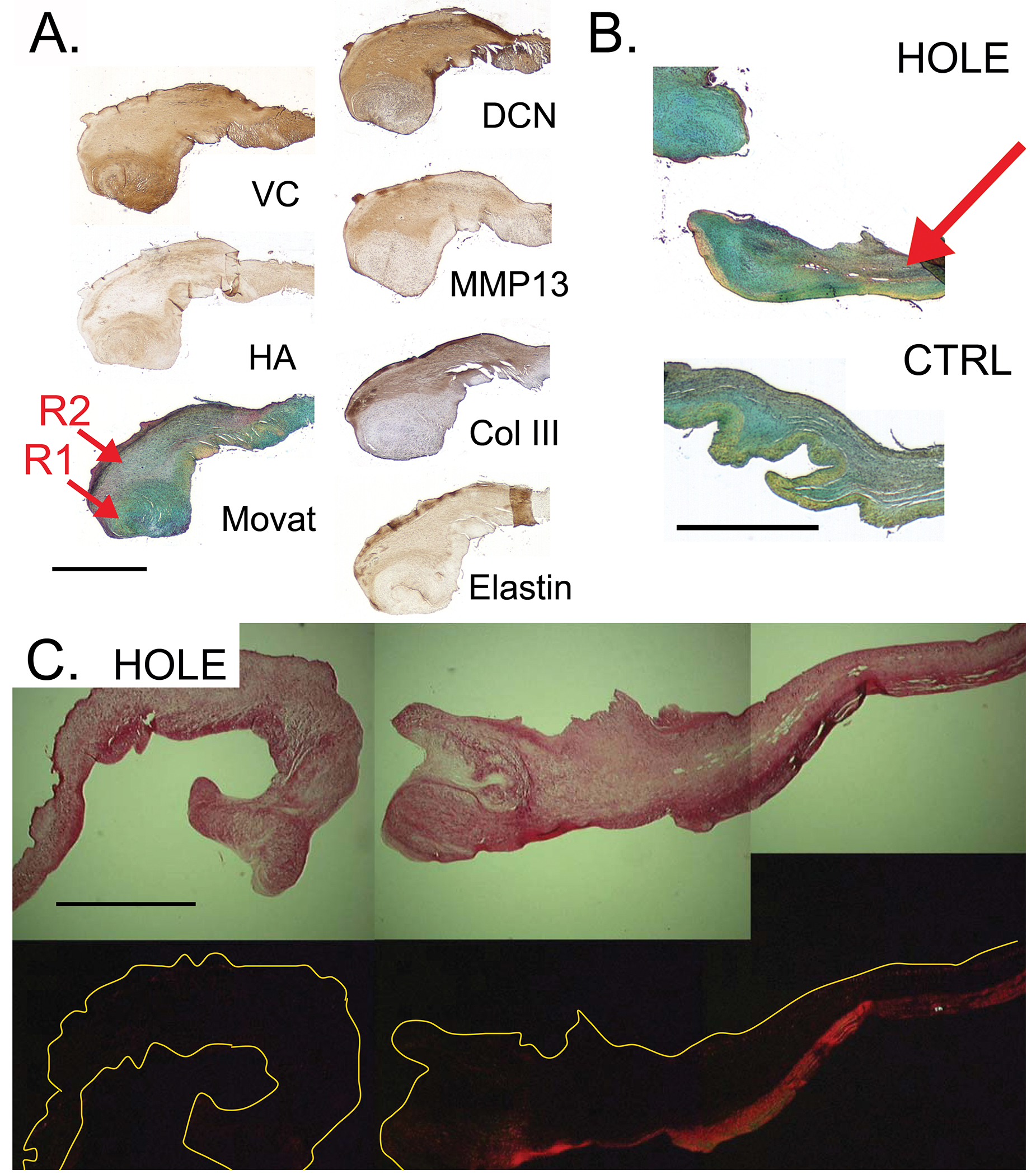
The details of valvular leaflet healing following valvuloplasty and leaflet perforation from endocarditis are poorly understood. In this study, the synthesis and turnover of valvular extracellular matrix due to healing of a critical sized wound was investigated. Twenty-nine sheep were randomized to either CTRL (n = 11) or HOLE (n = 18), in which a 2.8-4.8 mm diameter hole was punched in the posterior mitral leaflet. After 12 weeks, posterior leaflets were harvested and histologically stained to localize extracellular matrix components. Immunohistochemistry was also performed to assess matrix components and markers of matrix turnover. A semi-quantitative grading scale was used to quantify differences between HOLE and CTRL. After 12 weeks, the hole diameter was reduced by 71.3 ± 1.4 % (p < 0.001). Areas of remodeling surrounding the hole contained more activated cells, greater expression of proteoglycans, and markers of matrix turnover (prolyl 4-hydroxylase, metalloproteases, and lysyl oxidase, each p ≤ 0.025), along with fibrin accumulation. Two distinct remodeling regions were evident surrounding the hole, one directly bordering the hole rich in versican and hyaluronan and a second adjacent region with abundant collagen and elastic fiber turnover. The remodeling also caused reduced delineation between valve layers (p = 0.002), more diffuse staining of matrix components and markers of matrix turnover (p < 0.001), and disruption of the collagenous fibrosa. In conclusion, acute valve injury elicited distinct, heterogeneous alterations in valvular matrix composition and structure, resulting in partial wound closure. Because these changes could also affect leaflet mechanics and valve function, it will be important to determine their impact on healing wounds.
Keywords: Collagen; Mitral regurgitation; Mitral valve; Proteoglycans; Wound healing.
Conflict of interest statement
Conflict of Interest
The authors declare that they have no conflict of interest.
Figures
Similar articles
-
The effects of mitral regurgitation alone are sufficient for leaflet remodeling.Circulation. 2008 Sep 30;118(14 Suppl):S243-9. doi: 10.1161/CIRCULATIONAHA.107.757526. Circulation. 2008. PMID: 18824762 Free PMC article.
-
Significant changes in mitral valve leaflet matrix composition and turnover with tachycardia-induced cardiomyopathy.Circulation. 2009 Sep 15;120(11 Suppl):S112-9. doi: 10.1161/CIRCULATIONAHA.108.844159. Circulation. 2009. PMID: 19752355 Free PMC article.
-
Cellular and Extracellular Matrix Basis for Heterogeneity in Mitral Annular Contraction.Cardiovasc Eng Technol. 2015 Jun;6(2):151-9. doi: 10.1007/s13239-014-0209-3. Cardiovasc Eng Technol. 2015. PMID: 26195991 Free PMC article.
-
Emerging pathogenic mechanisms in human myxomatous mitral valve: lessons from past and novel data.Cardiovasc Pathol. 2013 Jul-Aug;22(4):245-50. doi: 10.1016/j.carpath.2012.11.001. Epub 2012 Dec 21. Cardiovasc Pathol. 2013. PMID: 23261354 Review.
-
The pathology of mitral valve prolapse.Herz. 1988 Aug;13(4):215-26. Herz. 1988. PMID: 3049284 Review.
Cited by
-
Association of matrix metalloprotease 1, 3, and 12 polymorphisms with rheumatic heart disease in a Chinese Han population.BMC Med Genet. 2018 Feb 20;19(1):27. doi: 10.1186/s12881-018-0538-4. BMC Med Genet. 2018. PMID: 29458338 Free PMC article.
-
The Epidermal Keratinocyte as a Therapeutic Target for Management of Diabetic Wounds.Int J Mol Sci. 2023 Feb 21;24(5):4290. doi: 10.3390/ijms24054290. Int J Mol Sci. 2023. PMID: 36901720 Free PMC article. Review.
-
Conditional deletion of RB1 in the Tie2 lineage leads to aortic valve regurgitation.PLoS One. 2018 Jan 5;13(1):e0190623. doi: 10.1371/journal.pone.0190623. eCollection 2018. PLoS One. 2018. PMID: 29304157 Free PMC article.
-
Macrophage-extracellular matrix interactions: Perspectives for tissue engineered heart valve remodeling.Front Cardiovasc Med. 2022 Sep 13;9:952178. doi: 10.3389/fcvm.2022.952178. eCollection 2022. Front Cardiovasc Med. 2022. PMID: 36176991 Free PMC article. Review.
References
-
- Dekker A, Black H, Von Lichtenberg F (1968) Mitral valve restenosis: a pathologic study. J Thorac Cardiovasc Surg 55:434–446 - PubMed
-
- Gillinov A, Cosgrove D, Lytle B, Taylor P, Stewart R, McCarthy P, Smedira N, Muehrcke D, Apperson-Hansen C, Loop F (1997) Reoperation for failure of mitral valve repair. J Thorac Cardiovasc Surg 113:467–473 - PubMed
-
- Briongos Figuero S, Moya Mur JL, Garcia-Lledo A, Centella T, Salido L, Acena Navarro A, Garcia Martin A, Garcia-Andrade I, Oliva E, Zamorano JL (2015) Predictors of persistent pulmonary hypertension after mitral valve replacement. Heart Vessels, in press. - PubMed
-
- I-Ida T, Tamura K, Tanaka S, Asano G (2001) [Blood vessels in normal and abnormal mitral valve leaflets]. J Nippon Med Sch 68:171–180 - PubMed
-
- Tamura K, Jones M, Yamada I, Ferrans VJ (2000) Wound healing in the mitral valve. J Heart Valve Dis 9:53–63 - PubMed
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
