

The HysNiche trial: hysteroscopic resection of uterine caesarean scar defect (niche) in patients with abnormal bleeding, a randomised controlled trial
- PMID: 26563197
- PMCID: PMC4642644
- DOI: 10.1186/s12905-015-0260-8
The HysNiche trial: hysteroscopic resection of uterine caesarean scar defect (niche) in patients with abnormal bleeding, a randomised controlled trial
Abstract
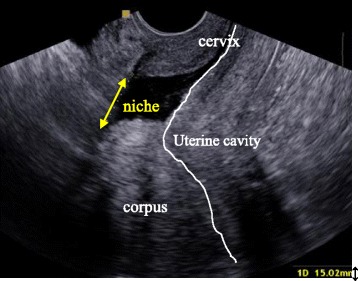
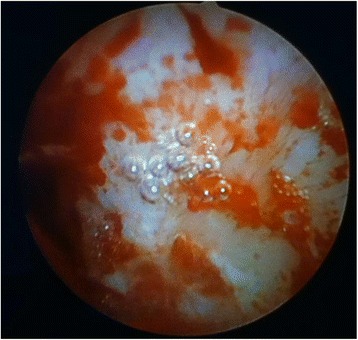
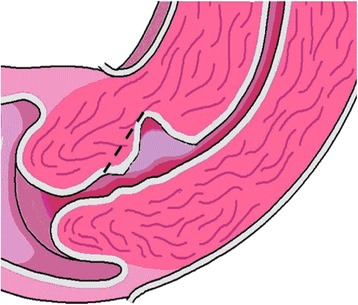
Background: A caesarean section (CS) can cause a defect or disruption of the myometrium at the site of the uterine scar, called a niche. In recent years, an association between a niche and postmenstrual spotting after a CS has been demonstrated. Hysteroscopic resection of these niches is thought to reduce spotting and menstrual pain. However, there are no randomised trials assessing the effectiveness of a hysteroscopic niche resection.
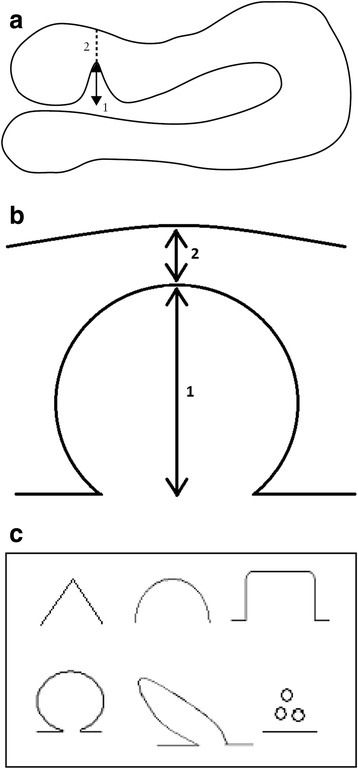
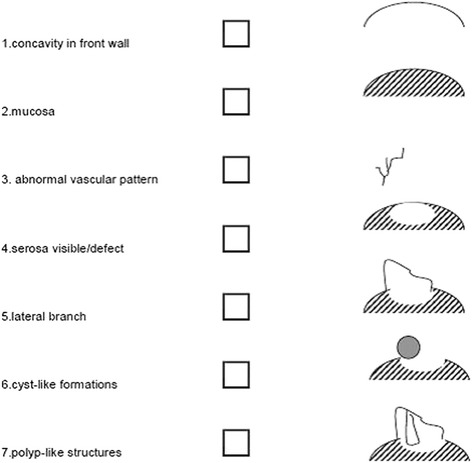
Methods/design: We planned a multicentre randomised trial comparing hysteroscopic niche resection to no intervention. We study women with postmenstrual spotting after a CS and a niche with a residual myometrium of at least 3 mm during sonohysterography. After informed consent is obtained, eligible women will be randomly allocated to hysteroscopic resection of the niche or expectant management for 6 months. The primary outcome is the number of days with postmenstrual spotting during one menstrual cycle 6 months after randomisation. Secondary outcomes are menstrual characteristics, menstruation related pain and experienced discomfort due to spotting or menstrual pain, quality of life, patient satisfaction, sexual function, urological symptoms, medical consultations, medication use, complications, lost productivity and medical costs. Measurements will be performed at baseline and at 3 and 6 months after randomisation. A cost-effectiveness analysis will be performed from a societal perspective at 6 months after randomisation.
Discussion: This trial will provide insight in the (cost)effectiveness of hysteroscopic resection of a niche versus expectant management in women who have postmenstrual spotting and a niche with sufficient residual myometrium to perform a hysteroscopic niche resection.
Trial registration: Dutch Trial Register NTR3269 . Registered 1 February 2012. ZonMw Grant number 80-82305-97-12030.
Figures

References
-
- Osterman MJ, Martin JA. Primary cesarean delivery rates, by state: results from the revised birth certificate, 2006–2012. Natl Vital Stat Rep. 2014;63:1–11. - PubMed
-
- Tian X, Wu J, Li B, Qin M, Qi J. Occurrence of cesarean section and related factors in 40 counties of China from 1978 to 2010. Zhonghua Yu Fang Yi Xue Za Zhi. 2014;48:391–5. - PubMed
Publication types
MeSH terms
Associated data
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
