

Clinical and economic consequences of first-year urinary tract infections, sepsis, and pneumonia in contemporary kidney transplantation practice
- PMID: 26563524
- PMCID: PMC4805426
- DOI: 10.1111/tri.12711
Clinical and economic consequences of first-year urinary tract infections, sepsis, and pneumonia in contemporary kidney transplantation practice
Abstract
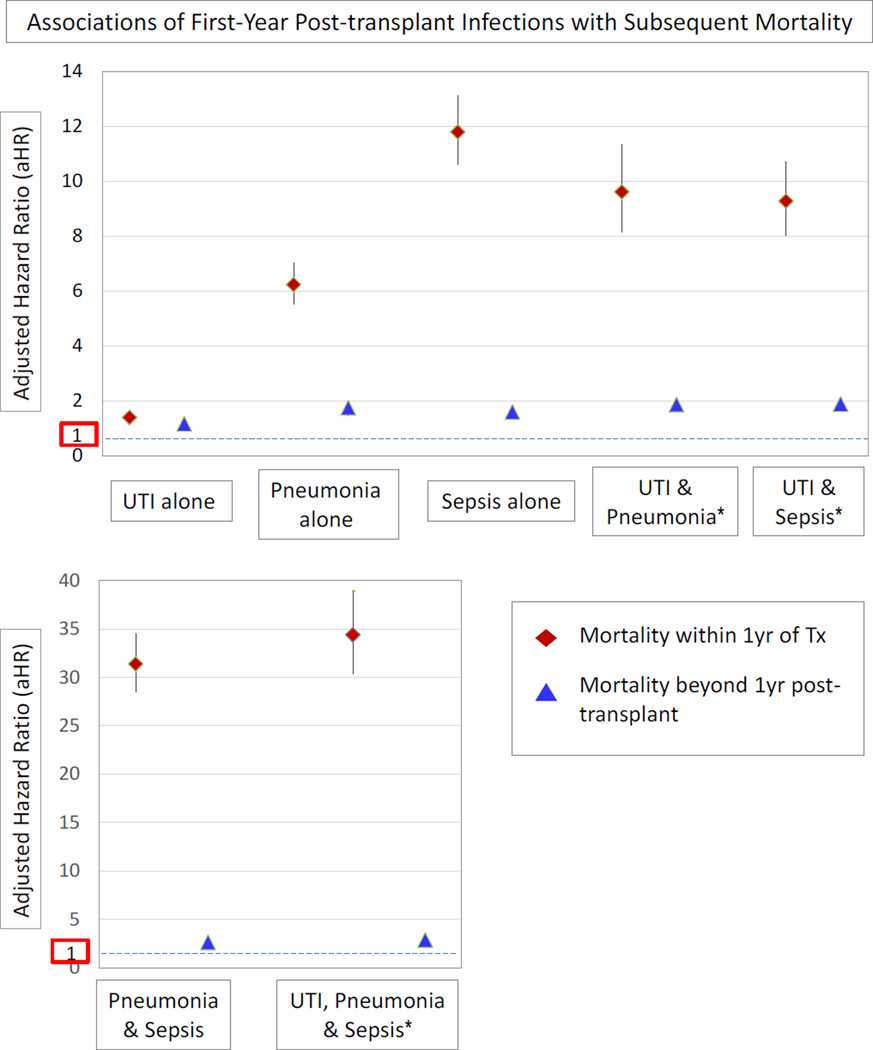
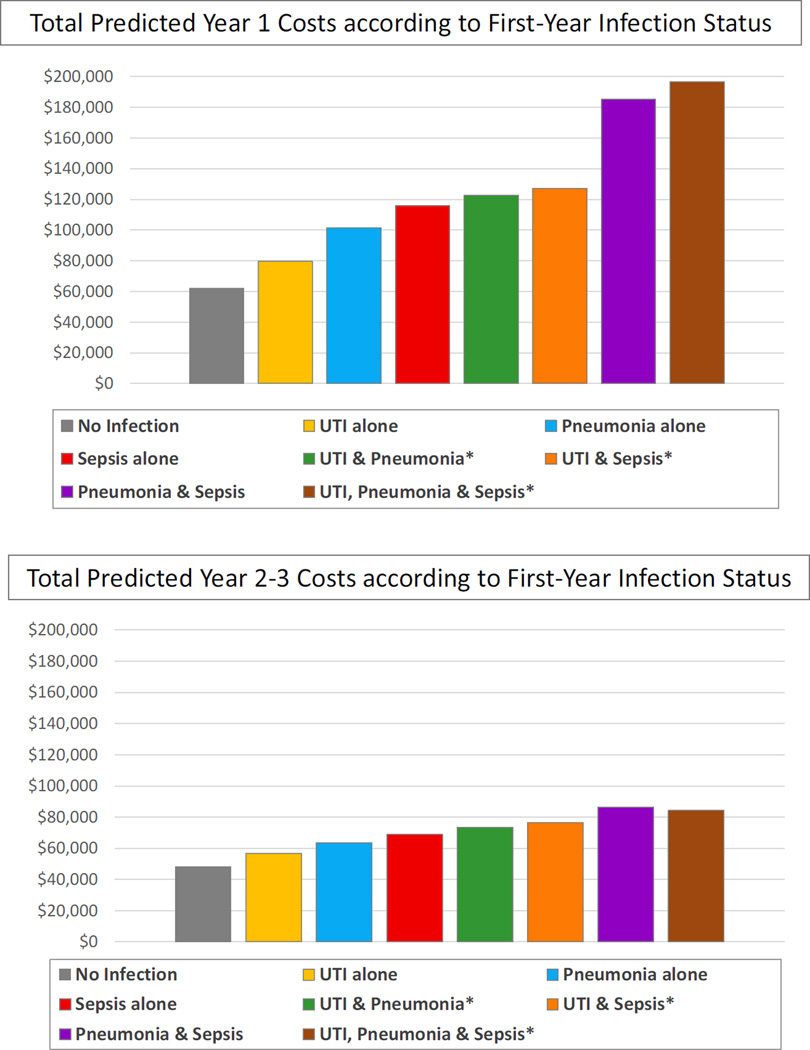
We examined United States Renal Data System registry records for Medicare-insured kidney transplant recipients in 2000-2011 to study the clinical and cost impacts of urinary tract infections (UTI), pneumonia, and sepsis in the first year post-transplant among a contemporary, national cohort. Infections were identified by billing diagnostic codes. Among 60 702 recipients, 45% experienced at least one study infection in the first year post-transplant, including UTI in 32%, pneumonia in 13%, and sepsis in 12%. Older recipient age, female sex, diabetic kidney failure, nonstandard criteria organs, sirolimus-based immunosuppression, and steroids at discharge were associated with increased risk of first-year infections. By time-varying, multivariate Cox regression, all study infections predicted increased first-year mortality, ranging from 41% (aHR 1.41, 95% CI 1.25-1.56) for UTI alone, 6- to 12-fold risk for pneumonia or sepsis alone, to 34-fold risk (aHR 34.38, 95% CI 30.35-38.95) for those with all three infections. Infections also significantly increased first-year costs, from $17 691 (standard error (SE) $591) marginal cost increase for UTI alone, to approximately $40 000-$50 000 (SE $1054-1238) for pneumonia or sepsis alone, to $134 773 (SE $1876) for those with UTI, pneumonia, and sepsis. Clinical and economic impacts persisted in years 2-3 post-transplant. Early infections reflect important targets for management protocols to improve post-transplant outcomes and reduce costs of care.
Keywords: economics; infections; kidney transplantation; medicare; registries.
© 2015 Steunstichting ESOT.
Conflict of interest statement
Figures
References
-
- Nankivell BJ, Alexander SI. Rejection of the kidney allograft. N Engl J Med. 2010;363(15):1451–1462. Epub 2010/10/12. - PubMed
-
- Lentine KL, Gheorghian A, Axelrod D, Kalsekar A, L'Italien G, Schnitzler MA. The implications of acute rejection for allograft survival in contemporary U.S. kidney transplantation. Transplantation. 2012;94(4):369–376. Epub 2012/07/28. - PubMed
-
- Lodhi SA, Lamb KE, Meier-Kriesche HU. Solid organ allograft survival improvement in the United States: the long-term does not mirror the dramatic short-term success. American journal of transplantation : official journal of the American Society of Transplantation and the American Society of Transplant Surgeons. 2011;11(6):1226–1235. Epub 2011/05/14. - PubMed
-
- Matas AJ, Smith JM, Skeans MA, Thompson B, Gustafson SK, Stewart DE, et al. OPTN/SRTR 2013 Annual Data Report: kidney. Am J Transplant. 2015;15(Suppl 2):1–34. Epub 2015/01/30. - PubMed
-
- Horwedel TA, Bowman LJ, Saab G, Brennan DC. Benefits of sulfamethoxazole-trimethoprim prophylaxis on rates of sepsis after kidney transplant. Transplant infectious disease : an official journal of the Transplantation Society. 2014;16(2):261–269. Epub 2014/03/14. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
