

Does inferior vena cava respiratory variability predict fluid responsiveness in spontaneously breathing patients?
- PMID: 26563768
- PMCID: PMC4643539
- DOI: 10.1186/s13054-015-1100-9
Does inferior vena cava respiratory variability predict fluid responsiveness in spontaneously breathing patients?
Abstract
Introduction: We have almost no information concerning the value of inferior vena cava (IVC) respiratory variations in spontaneously breathing ICU patients (SBP) to predict fluid responsiveness.
Methods: SBP with clinical fluid need were included prospectively in the study. Echocardiography and Doppler ultrasound were used to record the aortic velocity-time integral (VTI), stroke volume (SV), cardiac output (CO) and IVC collapsibility index (cIVC) ((maximum diameter (IVCmax)- minimum diameter (IVCmin))/ IVCmax) at baseline, after a passive leg-raising maneuver (PLR) and after 500 ml of saline infusion.
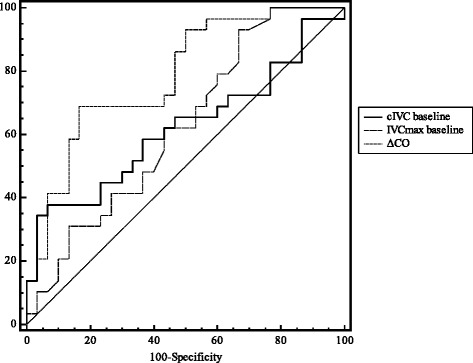
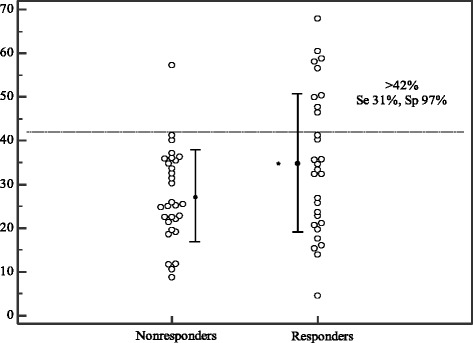
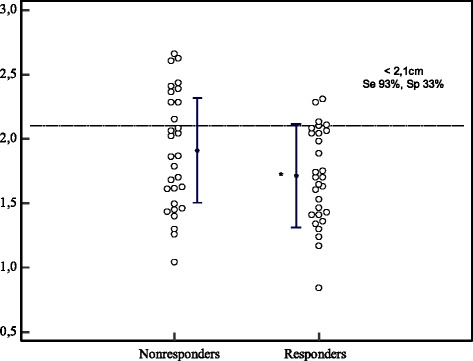
Results: Fifty-nine patients (30 males and 29 females; 57 ± 18 years-old) were included in the study. Of these, 29 (49 %) were considered to be responders (≥10 % increase in CO after fluid infusion). There were no significant differences between responders and nonresponders at baseline, except for a higher aortic VTI in nonresponders (16 cm vs. 19 cm, p = 0.03). Responders had a lower baseline IVCmin than nonresponders (11 ± 5 mm vs. 14 ± 5 mm, p = 0.04) and more marked IVC variations (cIVC: 35 ± 16 vs. 27 ± 10 %, p = 0.04). Prediction of fluid-responsiveness using cIVC and IVCmax was low (area under the curve for cIVC at baseline 0.62 ± 0.07; 95 %, CI 0.49-0.74 and for IVCmax at baseline 0.62 ± 0.07; 95 % CI 0.49-0.75). In contrast, IVC respiratory variations >42 % in SBP demonstrated a high specificity (97 %) and a positive predictive value (90 %) to predict an increase in CO after fluid infusion.
Conclusions: In SBP with suspected hypovolemia, vena cava size and respiratory variability do not predict fluid responsiveness. In contrast, a cIVC >42 % may predict an increase in CO after fluid infusion.
Figures
References
-
- National Heart, Lung, and Blood Institute Acute Respiratory Distress Syndrome (ARDS) Clinical Trials Network. Wiedemann HP, Wheeler AP, Bernard GR, Thompson BT, Hayden D, et al. Comparison of two fluid-management strategies in acute lung injury. N Engl J Med. 2006;354(24):2564–75. doi: 10.1056/NEJMoa062200. - DOI - PubMed
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
