

Cerebrolysin and Recovery After Stroke (CARS): A Randomized, Placebo-Controlled, Double-Blind, Multicenter Trial
- PMID: 26564102
- PMCID: PMC4689177
- DOI: 10.1161/STROKEAHA.115.009416
Cerebrolysin and Recovery After Stroke (CARS): A Randomized, Placebo-Controlled, Double-Blind, Multicenter Trial
Abstract
Background and purpose: The aim of this trial was to investigate whether stroke patients who receive Cerebrolysin show improved motor function in the upper extremities at day 90 compared with patients who receive a placebo.
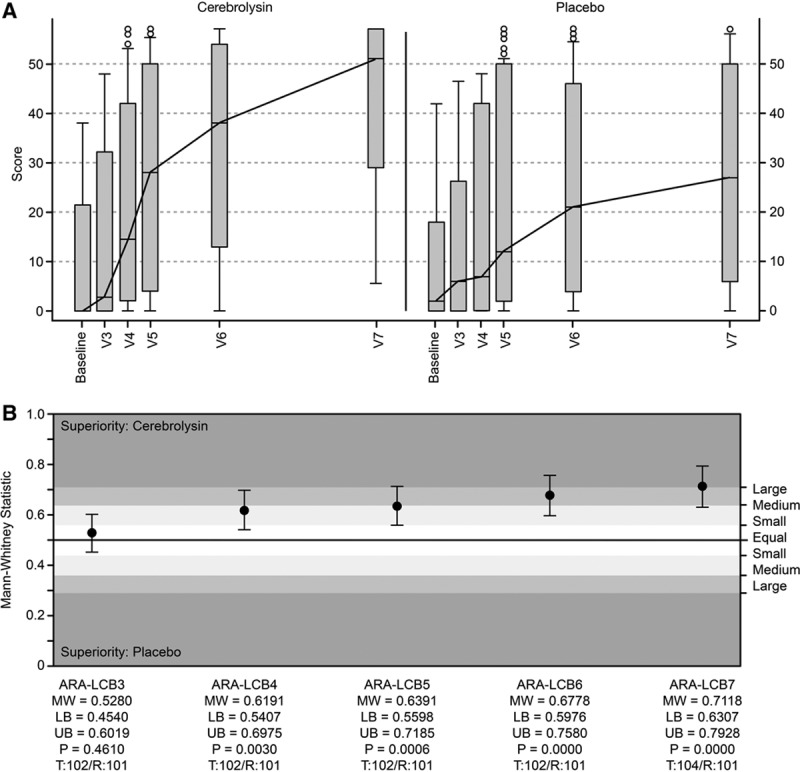
Methods: This study was a prospective, randomized, double-blind, placebo-controlled, multicenter, parallel-group study. Patients were treated with Cerebrolysin (30 mL/d) or a placebo (saline) once daily for 21 days, beginning at 24 to 72 hours after stroke onset. The patients also participated in a standardized rehabilitation program for 21 days that was initiated within 72 hours after stroke onset. The primary end point was the Action Research Arm Test score on day 90.
Results: The nonparametric effect size on the Action Research Arm Test score on day 90 indicated a large superiority of Cerebrolysin compared with the placebo (Mann-Whitney estimator, 0.71; 95% confidence interval, 0.63-0.79; P<0.0001). The multivariate effect size on global status, as assessed using 12 different outcome scales, indicated a small-to-medium superiority of Cerebrolysin (Mann-Whitney estimator, 0.62; 95% confidence interval, 0.58-0.65; P<0.0001). The rate of premature discontinuation was <5% (3.8%). Cerebrolysin was safe and well tolerated.
Conclusions: Cerebrolysin had a beneficial effect on function and global outcome in early rehabilitation patients after stroke. Its safety was comparable with that of the placebo, suggesting a favorable benefit/risk ratio. Because this study was exploratory and had a relatively small sample size, the results should be confirmed in a large-scale, randomized clinical trial.
Clinical trial registration: URL: http://www.clinicaltrialsregister.eu. Unique identifier: 2007-000870-21.
Keywords: Cerebrolysin; randomized, double-blind, placebo-controlled trial; recovery of function; rehabilitation; stroke.
© 2015 The Authors.
Figures


Comment in
-
Letter by Rezaei and Arjmand Regarding Article, "Cerebrolysin and Recovery After Stroke (CARS): A Randomized, Placebo-Controlled, Double-Blind, Multicenter Trial".Stroke. 2016 May;47(5):e90. doi: 10.1161/STROKEAHA.116.012979. Epub 2016 Apr 7. Stroke. 2016. PMID: 27056986 No abstract available.
References
-
- Murray CJ, Lopez AD. Measuring the global burden of disease. N Engl J Med. 2013;369:448–457. doi: 10.1056/NEJMra1201534. - PubMed
-
- Lozano R, Naghavi M, Foreman K, Lim S, Shibuya K, Aboyans V, et al. Global and regional mortality from 235 causes of death for 20 age groups in 1990 and 2010: a systematic analysis for the Global Burden of Disease Study 2010. Lancet. 2012;380:2095–2128. doi: 10.1016/S0140-6736(12)61728-0. - PMC - PubMed
-
- Wardlaw JM, Murray V, Berge E, del Zoppo GJ. Thrombolysis for acute ischemic stroke, update August 2014. Stroke. 2014;45:e222–e225. doi: 10.1161/STROKEAHA.114.007024.
-
- Pierot L, Soize S, Benaissa A, Wakhloo AK. Techniques for endovascular treatment of acute ischemic stroke: from intra-arterial fibrinolytics to stent-retrievers. Stroke. 2015;46:909–914. doi: 10.1161/STROKEAHA.114.007935. - PubMed
-
- Berkhemer OA, Fransen PS, Beumer D, van den Berg LA, Lingsma HF, et al. MR CLEAN Investigators. A randomized trial of intraarterial treatment for acute ischemic stroke. N Engl J Med. 2015;372:11–20. doi: 10.1056/NEJMoa1411587. - PubMed
Publication types
MeSH terms
Substances
Associated data
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
