

Examining the Association Between Comorbidity Indexes and Functional Status in Hospitalized Medicare Fee-for-Service Beneficiaries
- PMID: 26564253
- PMCID: PMC4752680
- DOI: 10.2522/ptj.20150039
Examining the Association Between Comorbidity Indexes and Functional Status in Hospitalized Medicare Fee-for-Service Beneficiaries
Abstract
Background: Medicare data from acute hospitals do not contain information on functional status. This lack of information limits the ability to conduct rehabilitation-related health services research.
Objective: The purpose of this study was to examine the associations between 5 comorbidity indexes derived from acute care claims data and functional status assessed at admission to an inpatient rehabilitation facility (IRF). Comorbidity indexes included tier comorbidity, Functional Comorbidity Index (FCI), Charlson Comorbidity Index, Elixhauser Comorbidity Index, and Hierarchical Condition Category (HCC).
Design: This was a retrospective cohort study.
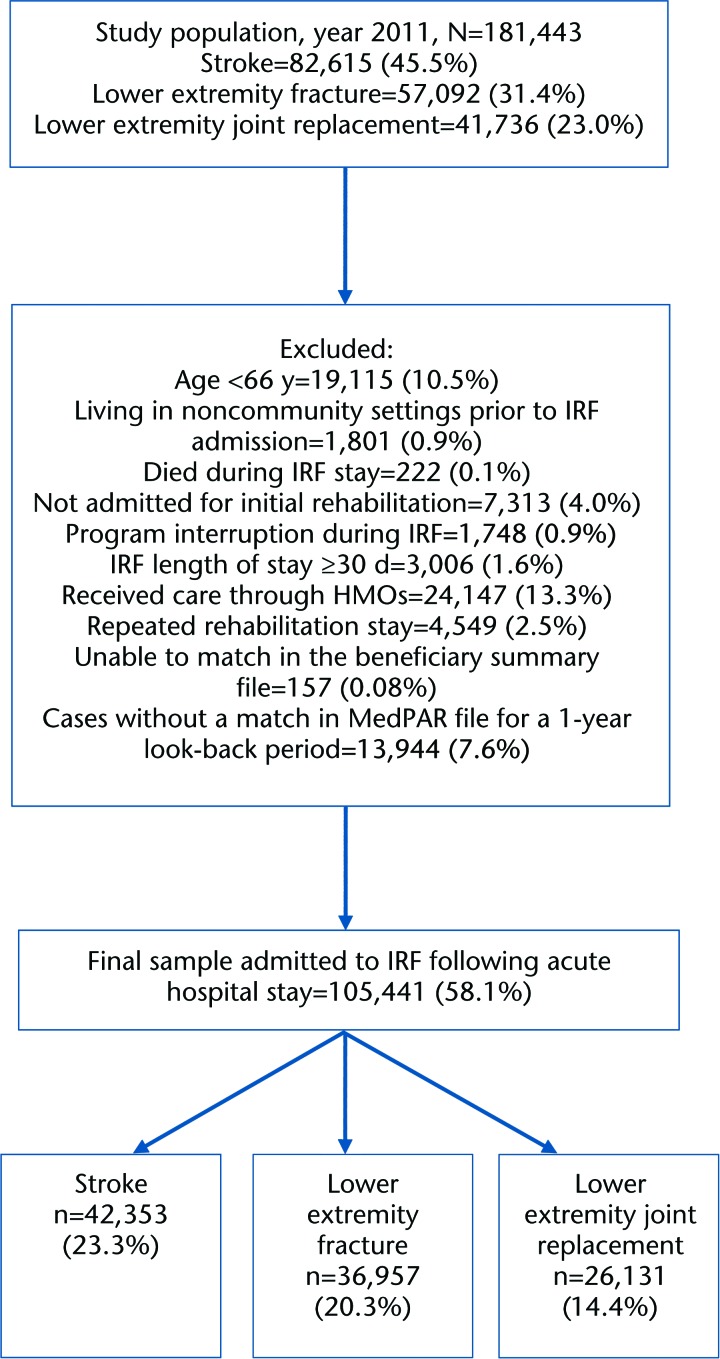
Methods: Medicare beneficiaries with stroke, lower extremity joint replacement, and lower extremity fracture discharged to an IRF in 2011 were studied (N=105,441). Data from the beneficiary summary file, Medicare Provider Analysis and Review (MedPAR) file, and Inpatient Rehabilitation Facility-Patient Assessment Instrument (IRF-PAI) file were linked. Inpatient rehabilitation facility admission functional status was used as a proxy for acute hospital discharge functional status. Separate linear regression models for each impairment group were developed to assess the relationships between the comorbidity indexes and functional status. Base models included age, sex, race/ethnicity, disability, dual eligibility, and length of stay. Subsequent models included individual comorbidity indexes. Values of variance explained (R(2)) with each comorbidity index were compared.
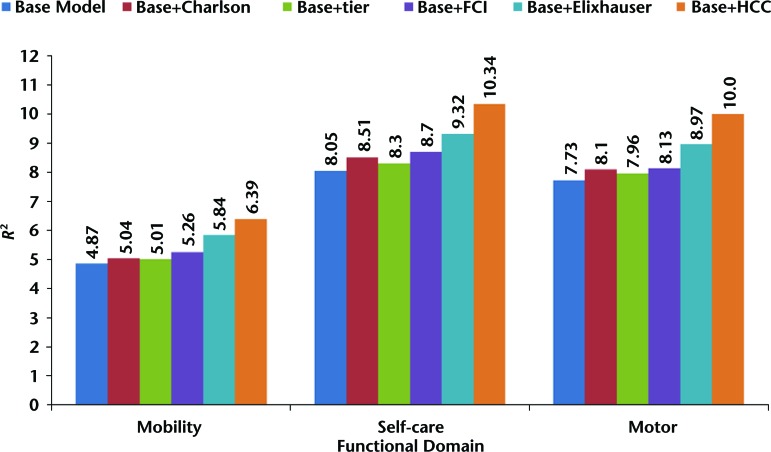
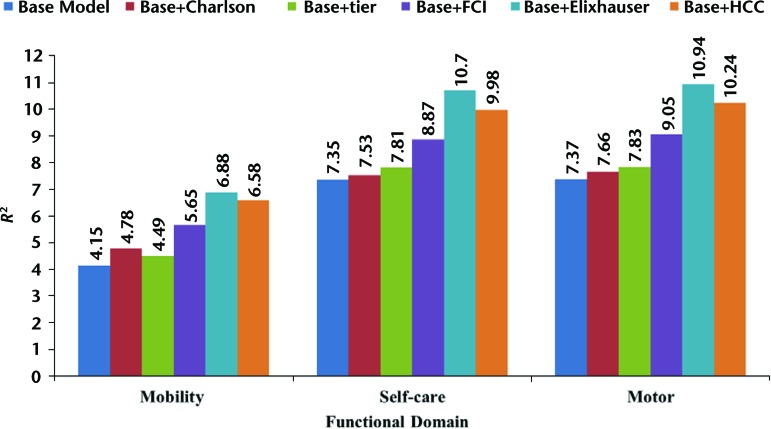
Results: Base models explained 7.7% of the variance in motor function ratings for stroke, 3.8% for joint replacement, and 7.3% for fracture. The R(2) increased marginally when comorbidity indexes were added to base models for stroke, joint replacement, and fracture: Charlson Comorbidity Index (0.4%, 0.5%, 0.3%), tier comorbidity (0.2%, 0.6%, 0.5%), FCI (0.4%, 1.2%, 1.6%), Elixhauser Comorbidity Index (1.2%, 1.9%, 3.5%), and HCC (2.2%, 2.1%, 2.8%).
Limitation: Patients from 3 impairment categories were included in the sample.
Conclusions: The 5 comorbidity indexes contributed little to predicting functional status. The indexes examined were not useful as proxies for functional status in the acute settings studied.
© 2016 American Physical Therapy Association.
Figures

References
-
- Graf C. Functional decline in hospitalized older adults. Am J Nurs. 2006;106:58–67. - PubMed
-
- Hoenig HM, Rubenstein LZ. Hospital-associated deconditioning and dysfunction. J Am Geriatr Soc. 1991;39:220–222. - PubMed
-
- Brown CJ, Friedkin RJ, Inouye SK. Prevalence and outcomes of low mobility in hospitalized older patients. J Am Geriatr Soc. 2004;52:1263–1270. - PubMed
-
- Fields SD, MacKenzie CR, Charlson ME, Sax FL. Cognitive impairment: can it predict the course of hospitalized patients? J Am Geriatr Soc. 1986;34:579–585. - PubMed
-
- Inouye SK, Peduzzi PN, Robison JT, et al. Importance of functional measures in predicting mortality among older hospitalized patients. JAMA. 1998;279:1187–1193. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
