

Utility and Significance of Gadolinium-Based Contrast Enhancement in Posterior Reversible Encephalopathy Syndrome
- PMID: 26564441
- PMCID: PMC5584787
- DOI: 10.3174/ajnr.A4563
Utility and Significance of Gadolinium-Based Contrast Enhancement in Posterior Reversible Encephalopathy Syndrome
Abstract
Background and purpose: Posterior reversible encephalopathy syndrome is a clinicoradiologic syndrome. Literature regarding associated factors and the prognostic significance of contrast enhancement in posterior reversible encephalopathy syndrome is sparse. This study set out to evaluate an association between the presence of enhancement in posterior reversible encephalopathy syndrome and various clinical factors in a large series of patients with this syndrome.
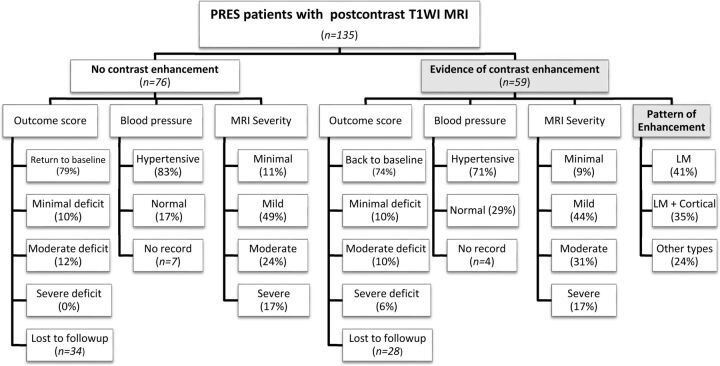
Materials and methods: From an MR imaging report search that yielded 176 patients with clinically confirmed posterior reversible encephalopathy syndrome between 1997 and 2014, we identified 135 patients who had received gadolinium-based contrast. The presenting symptoms, etiology, clinical follow-up, and maximum systolic and diastolic blood pressures within 1 day of MR imaging were recorded. MRIs were reviewed for parenchymal hemorrhage, MR imaging severity, and the presence and pattern of contrast enhancement. Statistical analyses evaluated a correlation between any clinical features and the presence or pattern of enhancement.
Results: Of 135 included patients (67.4% females; age range, 7-82 years), 59 (43.7%) had contrast enhancement on T1-weighted MR imaging, the most common pattern being leptomeningeal (n = 24, 17.8%) or leptomeningeal plus cortical (n = 21, 15.6%). Clinical outcomes were available in 96 patients. No significant association was found between the presence or pattern of enhancement and any of the variables, including sex, age, symptom, MR imaging severity, blood pressure, or outcome (all P > .05 after Bonferroni correction).
Conclusions: The presence or pattern of enhancement in posterior reversible encephalopathy syndrome is not associated with any of the tested variables. However, an association was found between MR imaging severity and clinical outcome.
© 2016 by American Journal of Neuroradiology.
Figures
Comment in
-
Reply.AJNR Am J Neuroradiol. 2016 Sep;37(9):E59. doi: 10.3174/ajnr.A4872. Epub 2016 Jun 16. AJNR Am J Neuroradiol. 2016. PMID: 27313133 Free PMC article. No abstract available.
-
Utility and Significance of Gadolinium-Based Contrast Enhancement in Posterior Reversible Encephalopathy Syndrome.AJNR Am J Neuroradiol. 2016 Sep;37(9):E58. doi: 10.3174/ajnr.A4847. Epub 2016 Jun 16. AJNR Am J Neuroradiol. 2016. PMID: 27313134 Free PMC article. No abstract available.
-
Reply.AJNR Am J Neuroradiol. 2016 Sep;37(9):E57. doi: 10.3174/ajnr.A4876. Epub 2016 Jun 30. AJNR Am J Neuroradiol. 2016. PMID: 27365327 Free PMC article. No abstract available.
-
The Clinical Outcome of Posterior Reversible Encephalopathy Syndrome.AJNR Am J Neuroradiol. 2016 Sep;37(9):E55-6. doi: 10.3174/ajnr.A4853. Epub 2016 Jun 30. AJNR Am J Neuroradiol. 2016. PMID: 27365328 Free PMC article. No abstract available.
References
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical