Mechanical Thrombectomy for Isolated M2 Occlusions: A Post Hoc Analysis of the STAR, SWIFT, and SWIFT PRIME Studies
- PMID: 26564442
- PMCID: PMC7960159
- DOI: 10.3174/ajnr.A4591
Mechanical Thrombectomy for Isolated M2 Occlusions: A Post Hoc Analysis of the STAR, SWIFT, and SWIFT PRIME Studies
Abstract
Background and purpose: Mechanical thrombectomy is beneficial for patients with acute ischemic stroke and a proximal anterior occlusion, but it is unclear if these results can be extrapolated to patients with an M2 occlusion. The purpose of this study was to examine the technical aspects, safety, and outcomes of mechanical thrombectomy with a stent retriever in patients with an isolated M2 occlusion who were included in 3 large multicenter prospective studies.
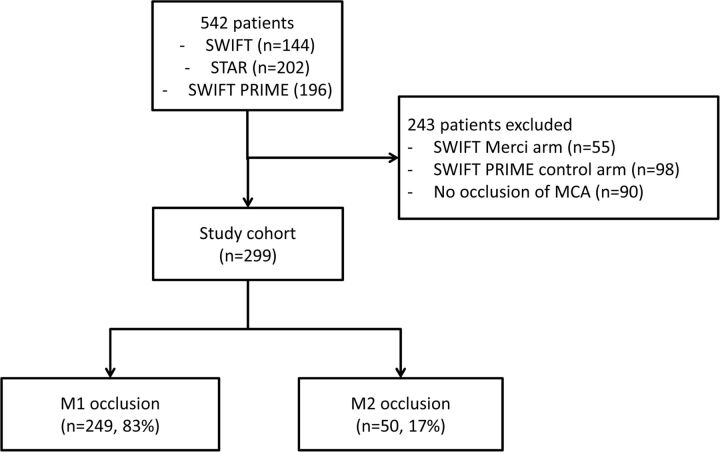
Materials and methods: We included patients from the Solitaire Flow Restoration Thrombectomy for Acute Revascularization (STAR), Solitaire With the Intention For Thrombectomy (SWIFT), and Solitaire With the Intention for Thrombectomy as Primary Endovascular Treatment (SWIFT PRIME) studies, 3 large multicenter prospective studies on thrombectomy for ischemic stroke. We compared outcomes and technical details of patients with an M2 with those with an M1 occlusion. All patients were treated with a stent retriever. Imaging data and outcomes were scored by an independent core laboratory. Successful reperfusion was defined as modified Thrombolysis in Cerebral Infarction score of 2b/3.
Results: We included 50 patients with an M2 and 249 patients with an M1 occlusion. Patients with an M2 occlusion were older (mean age, 71 versus 67 years; P = .04) and had a lower NIHSS score (median, 13 versus 17; P < .001) compared with those with an M1 occlusion. Procedural time was nonsignificantly shorter in patients with an M2 occlusion (median, 29 versus 35 minutes; P = .41). The average number of passes with a stent retriever was also nonsignificantly lower in patients with an M2 occlusion (mean, 1.4 versus 1.7; P = .07). There were no significant differences in successful reperfusion (85% versus 82%, P = .82), symptomatic intracerebral hemorrhages (2% versus 2%, P = 1.0), device-related serious adverse events (6% versus 4%, P = .46), or modified Rankin Scale score 0-2 at follow-up (60% versus 56%, P = .64).
Conclusions: Endovascular reperfusion therapy appears to be feasible in selected patients with ischemic stroke and an M2 occlusion.
© 2016 by American Journal of Neuroradiology.