

The Classification for Early-onset Scoliosis (C-EOS) Correlates With the Speed of Vertical Expandable Prosthetic Titanium Rib (VEPTR) Proximal Anchor Failure
- PMID: 26566066
- PMCID: PMC5664192
- DOI: 10.1097/BPO.0000000000000682
The Classification for Early-onset Scoliosis (C-EOS) Correlates With the Speed of Vertical Expandable Prosthetic Titanium Rib (VEPTR) Proximal Anchor Failure
Abstract
Background: The Classification for Early-onset Scoliosis (C-EOS) was developed by a consortium of early-onset scoliosis (EOS) surgeons. This study aims to examine if the C-EOS classification correlates with the speed (failure/unit time) of proximal anchor failure in EOS surgery patients.
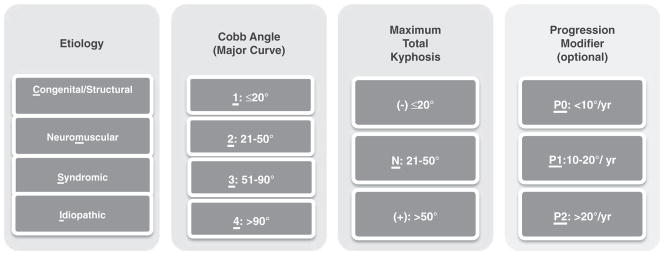
Methods: A total of 106 EOS patients were retrospectively queried from an EOS database. All patients were treated with vertical expandable prosthetic titanium rib and experienced proximal anchor failure. Patients were classified by the C-EOS, which includes a term for etiology [C: Congenital (54.2%), M: Neuromuscular (32.3%), S: Syndromic (8.3%), I: Idiopathic (5.2%)], major curve angle [1: ≤20 degrees (0%), 2: 21 to 50 degrees (15.6%), 3: 51 to 90 degrees (66.7%), 4: >90 degrees (17.7%)], and kyphosis ["-": ≤20 (13.5%), "N": 21 to 50 (42.7%), "+": >50 (43.8%)]. Outcome was measured by time and number of lengthenings to failure.
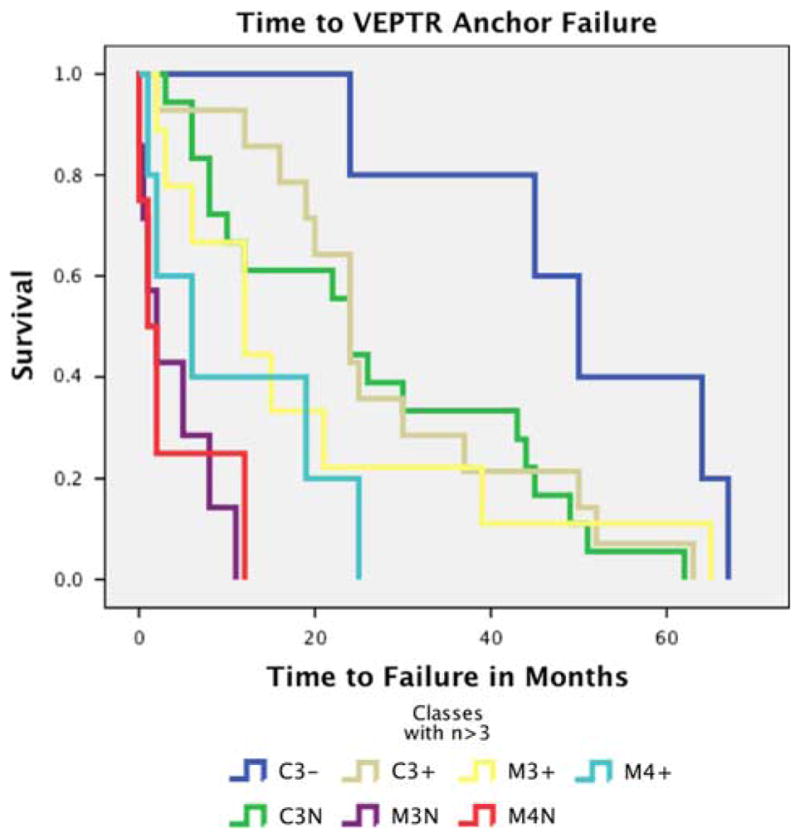
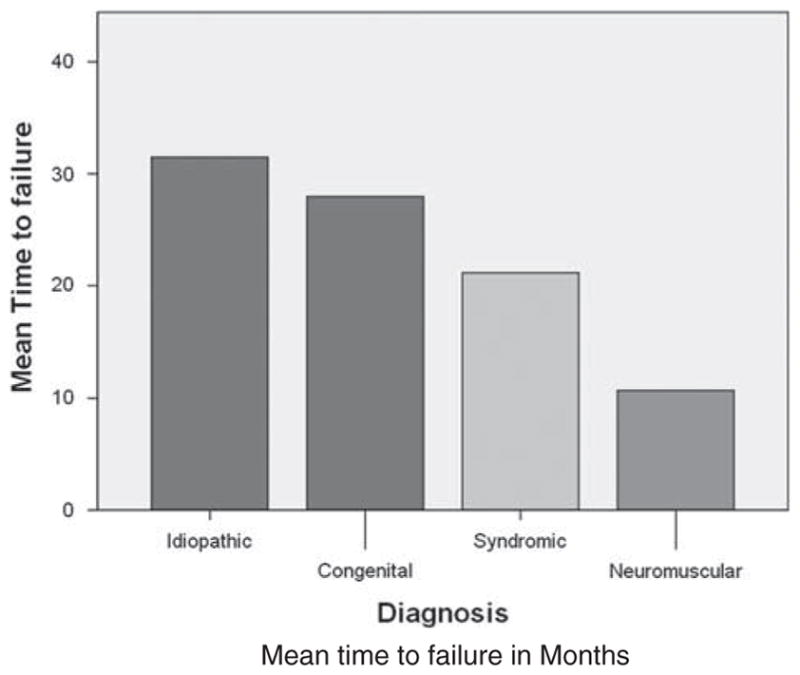
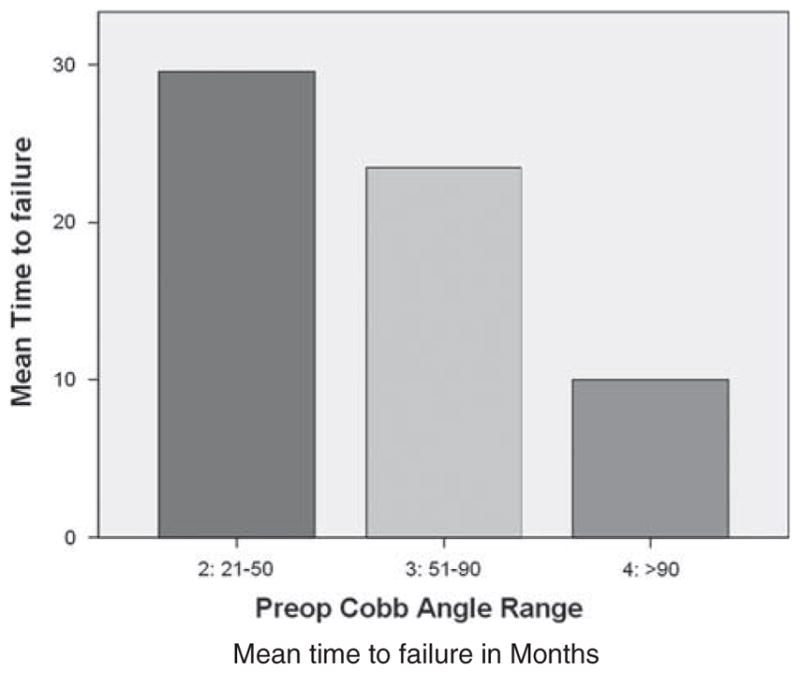
Results: Analyzing C-EOS classes with >3 subjects, survival analysis demonstrates that the C-EOS discriminates low, medium, and high speed of failure. The low speed of failure group consisted of congenital/51-90/hypokyphosis (C3-) class. The medium-speed group consisted of congenital/51-90/normal and hyperkyphosis (C3N, C3+), and neuromuscular/51-90/hyperkyphosis (M3+) classes. The high-speed group consisted of neuromuscular/51-90/normal kyphosis (M3N), and neuromuscular/>90/normal and hyperkyphosis (M4N, M4+) classes. Significant differences were found in time (P<0.05) and number of expansions (P<0.05) before failure between congenital and neuromuscular classes.As isolated variables, neuromuscular etiology experienced a significantly faster time to failure compared with patients with idiopathic (P<0.001) and congenital (P=0.026) etiology. Patients with a major curve angle >90 degrees demonstrated significantly faster speed of failure compared with patients with major curve angle 21 to 50 degrees (P=0.011).
Conclusions: The ability of the C-EOS to discriminate the speeds of failure of the various classification subgroups supports its validity and demonstrates its potential use in guiding decision making. Further experience with the C-EOS may allow more tailored treatment, and perhaps better outcomes of patients with EOS.
Level of evidence: Level III.
Conflict of interest statement
The remaining authors declare no conflicts of interest.
Figures
References
-
- Fernandes P, Weinstein SL. Natural history of early onset scoliosis. J Bone Joint Surg Am. 2007;89(suppl 1):21–33. - PubMed
-
- Chandran S, McCarthy J, Noonan K, et al. Early treatment of scoliosis with growing rods in children with severe spinal muscular atrophy: a preliminary report. J Pediatr Orthop. 2011;31:450–454. - PubMed
-
- Gillingham BL, Fan RA, Akbarnia BA. Early onset idiopathic scoliosis. J Am Acad Orthop Surg. 2006;14:101–112. - PubMed
-
- Hedequist D, Emans J. Congenital scoliosis: a review and update. J Pediatr Orthop. 2007;27:106–116. - PubMed
-
- Yang JS, McElroy MJ, Akbarnia BA, et al. Growing rods for spinal deformity: characterizing consensus and variation in current use. J Pediatr Orthop. 2010;30:264–270. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Research Materials
Miscellaneous