

Detection and Characterization of Metastatic Cancer Cells in the Mesogastrium of Gastric Cancer Patients
- PMID: 26566136
- PMCID: PMC4643961
- DOI: 10.1371/journal.pone.0142970
Detection and Characterization of Metastatic Cancer Cells in the Mesogastrium of Gastric Cancer Patients
Erratum in
-
Correction: Detection and Characterization of Metastatic Cancer Cells in the Mesogastrium of Gastric Cancer Patients.PLoS One. 2016 Jan 29;11(1):e0148681. doi: 10.1371/journal.pone.0148681. eCollection 2016. PLoS One. 2016. PMID: 26824866 Free PMC article. No abstract available.
Abstract
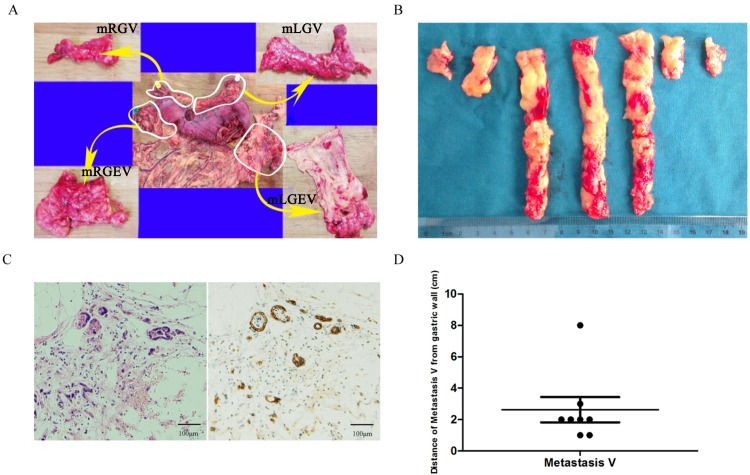
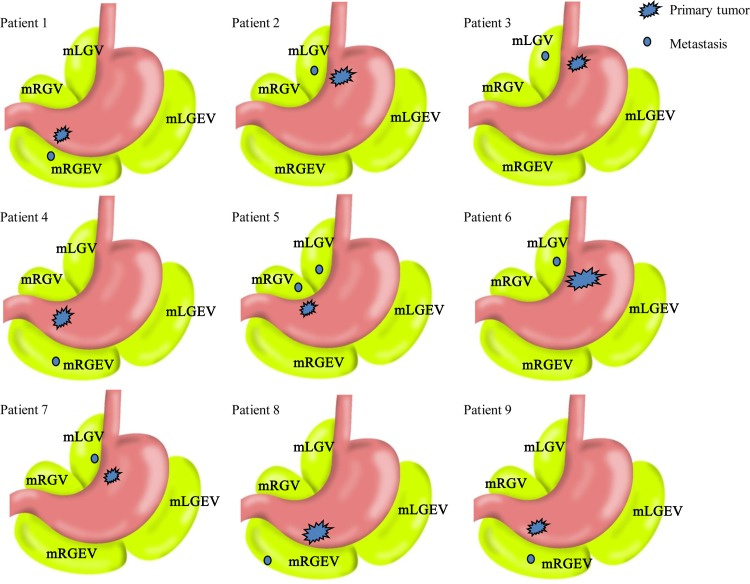
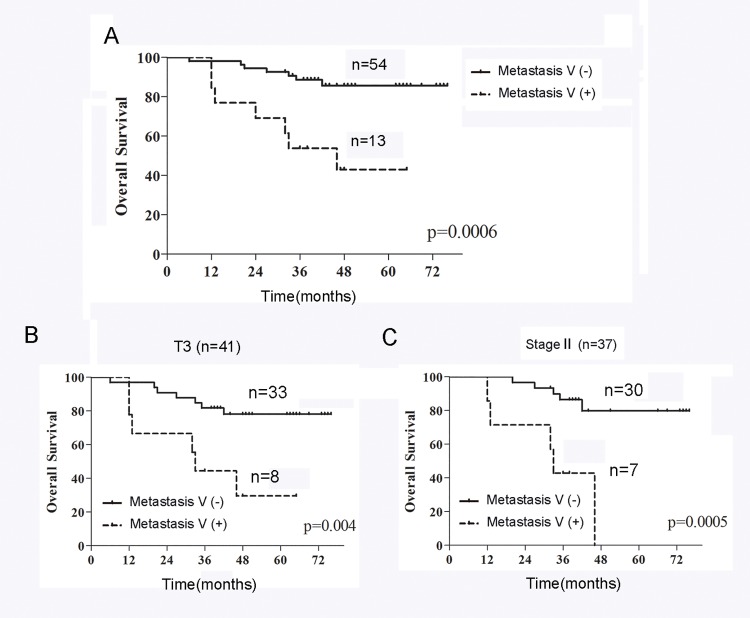
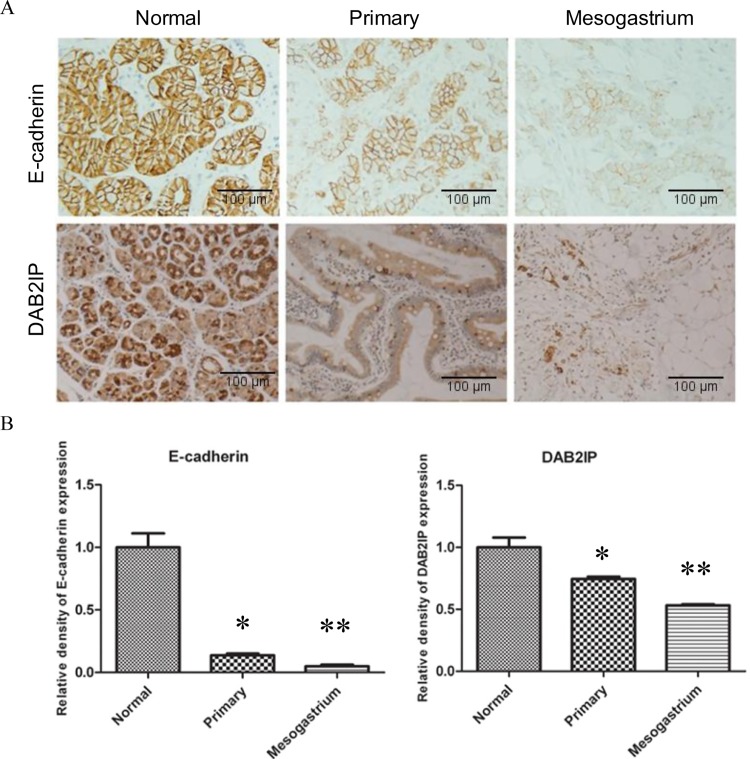
Gastric cancer is the second leading cause of cancer death worldwide. Here, we propose a novel type of tumor metastasis designated as Metastasis V in gastric cancer. Metastasis V is defined as the appearance of cancer cells in the mesogastrium with perigastric adipose tissue. To detect its incidence and characterize its clinic pathological features, large cross sectional tissue analysis of mesogastrium from 74 patients were used. Metastasis V was detected in 1 of 40 (2.5%) patients with early gastric cancer, 8 of 34 (24%) patients with advanced gastric cancer. The mean distance of Metastasis V from gastric wall was approximately 2.6 cm. Metastasis V was closely associated with tumor invasion depth, along with a number of positive lymph node metastasis. The prognosis of patients with Metastasis V was significantly (P<0.05) worse than those with tumor cell-free mesogastrium. These findings indicate that by using whole-sectional analysis, Metastasis V can be detected in the mesogastrium of gastric cancer patients, and also suggests that it may be a risk factor for patient survival after radical surgery.
Conflict of interest statement
Figures
References
-
- Dickson JL, Cunningham D. Systemic treatment of gastric cancer. Eur J Gastroenterol Hepatol. 2004, 16: 255–263. - PubMed
-
- Otsuji E, Kobayashi S, Okamoto K, Hagiwara A, Yamagishi H. Is timing of death from tumor recurrence predictable after curative resection for gastric cancer? World J Surg. 2001, 25: 1373–1376. - PubMed
-
- Heald RJ, Husband EM, Ryall RD. The mesorectum in rectal cancer surgery—the clue to pelvic recurrence? Br J Surg. 1982, 69: 613–616. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
