

How much is too much? Outcomes in patients using high-dose insulin glargine
- PMID: 26566714
- PMCID: PMC4738456
- DOI: 10.1111/ijcp.12747
How much is too much? Outcomes in patients using high-dose insulin glargine
Abstract
Background and objectives: Many patients with type 2 diabetes mellitus (T2DM) do not achieve glycaemic control targets on basal insulin regimens. This analysis investigated characteristics, clinical outcomes and impact of concomitant oral antidiabetes drugs (OADs) in patients with T2DM treated with high-dose insulin glargine.
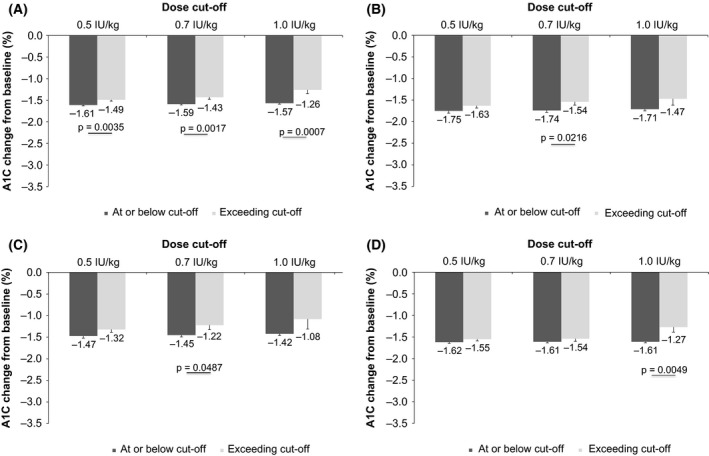
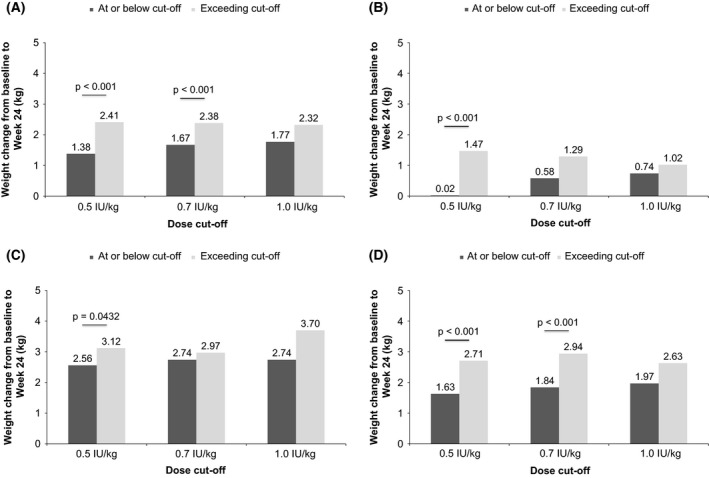
Methods: Patient-level data were pooled from 15 randomised, treat-to-target trials in patients with T2DM treated with insulin glargine ± OADs for ≥ 24 weeks. Data were stratified according to whether patients exceeded three insulin dose cut-off levels (> 0.5, > 0.7 and > 1.0 IU/kg). End-points included glycated haemoglobin A1c (A1C), fasting plasma glucose, body weight, and overall, nocturnal and severe hypoglycaemia.
Results: Data from 2837 insulin-naïve patients were analysed. Patients with insulin titrated beyond the three doses investigated had significantly higher baseline A1C levels and were younger, with shorter diabetes duration than those at/below cut-offs (p < 0.05 for all cut-offs); they also had greater weight gain (p < 0.001 for the > 0.5 and > 0.7 IU/kg cut-offs) than those who did not exceed the cut-offs, regardless of concomitant OAD. Patients on concomitant metformin alone had higher insulin doses at Week 24, but achieved greater reductions in A1C, less weight gain and lower hypoglycaemia rates than patients on a concomitant sulfonylurea or metformin plus a sulfonylurea, regardless of whether cut-offs were exceeded.
Conclusion: In patients with T2DM, increasing basal insulin doses above 0.5 IU/kg may not improve glycaemic control; treatment strategies targeting postprandial glucose control should be considered for such patients.
© 2015 Authors. International Journal of Clinical Practice Published by John Wiley & Sons Ltd.
Figures


References
-
- Inzucchi SE, Bergenstal RM, Buse JB et al. Management of hyperglycemia in type 2 diabetes, 2015: a patient‐centered approach: update to a position statement of the American Diabetes Association and the European Association for the Study of Diabetes. Diabetes Care 2015; 38: 140–9. - PubMed
-
- Garber AJ, Abrahamson MJ, Barzilay JI et al. AACE comprehensive diabetes management algorithm 2013. Endocr Pract 2013; 19: 327–36. - PubMed
-
- Mata‐Cases M, Benito‐Badorrey B, Roura‐Olmeda P et al. Clinical inertia in the treatment of hyperglycemia in type 2 diabetes patients in primary care. Curr Med Res Opin 2013; 29: 1495–502. - PubMed
-
- Reach G. Clinical inertia, uncertainty and individualized guidelines. Diabetes Metab 2014; 40: 241–5. - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical