

B Cell Reconstitution after Rituximab Treatment in Idiopathic Nephrotic Syndrome
- PMID: 26567244
- PMCID: PMC4884116
- DOI: 10.1681/ASN.2015050523
B Cell Reconstitution after Rituximab Treatment in Idiopathic Nephrotic Syndrome
Abstract
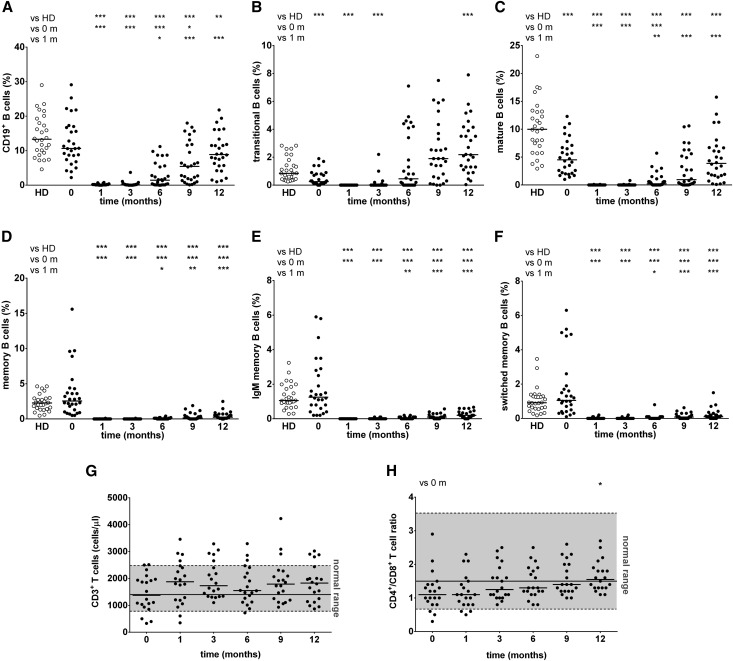
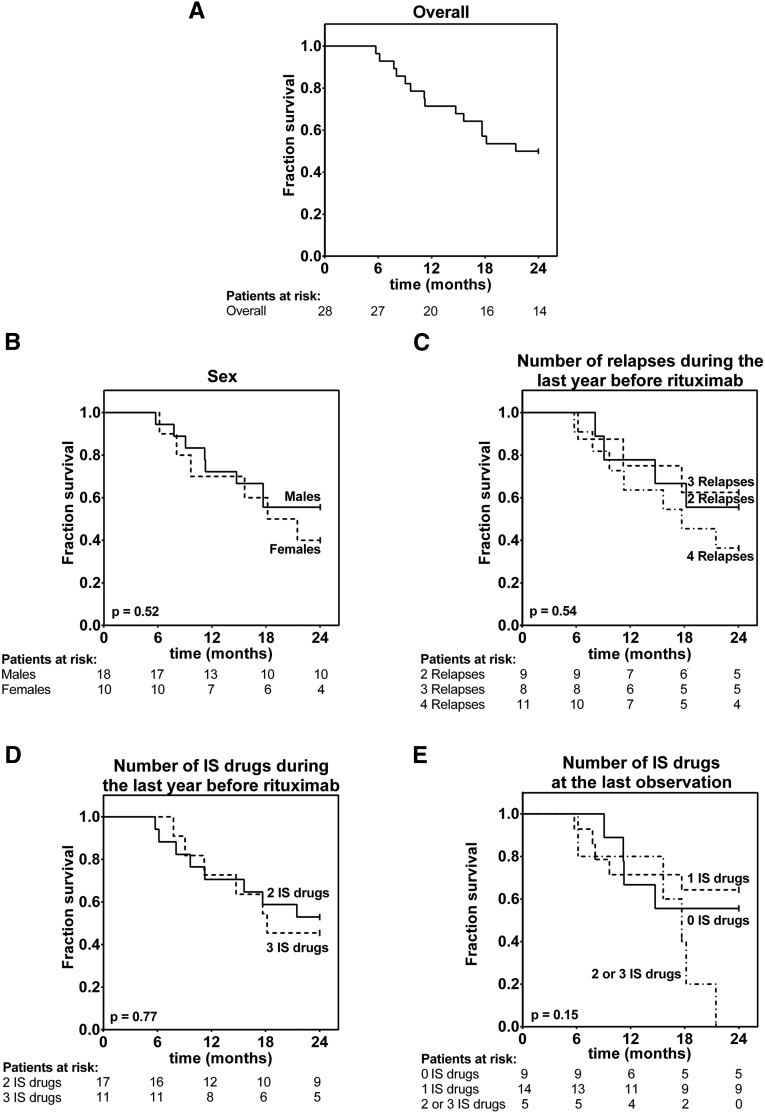
The pathogenesis of nephrotic syndrome is unclear. However, the efficacy of rituximab, a B cell-depleting antibody, in nephrotic syndrome suggests a pathogenic role of B cells. In this retrospective study, we determined by flow cytometry levels of B and T cell subpopulations before and after rituximab infusion in 28 pediatric patients with frequently relapsing or steroid-dependent nephrotic syndrome. At baseline, patients had lower median percentages of transitional and mature B cells than age-matched healthy controls (P<0.001). Rituximab induced full depletion of B cells (<1% of lymphocytes). At 1 year, most patients exhibited complete total and mature B cell recovery, whereas memory B cell subsets remained significantly depleted. Total T cell concentration did not change with rituximab, whereas the CD4(+)/CD8(+) T cell ratio tended to increase. Fourteen patients relapsed within 24 months, with a median follow-up of 11.2 months (interquartile range, 8-17.7 months). We observed no difference at baseline between nonrelapsing and relapsing patients in several clinical parameters and cell subset concentrations. Reconstitution of all memory B cell subpopulations, number of immunosuppressive drugs, and dose of tacrolimus during the last 4 months of follow-up were predictive of relapse in univariate Cox regression analysis. However, only delayed reconstitution of switched memory B cells, independent of immunosuppressive treatment, was protective against relapse in multivariate (P<0.01) and receiver operator characteristic (P<0.01 for percentage of lymphocytes; P=0.02 for absolute count) analyses. Evaluation of switched memory B cell recovery after rituximab may be useful for predicting relapse in patients with nephrotic syndrome.
Keywords: clinical immunology; glomerular disease; idiopathic nephrotic syndrome; immunosuppression; lymphocytes.
Copyright © 2016 by the American Society of Nephrology.
Figures



Comment in
-
Busy Bs.J Am Soc Nephrol. 2016 Jun;27(6):1584-6. doi: 10.1681/ASN.2015101171. Epub 2015 Nov 30. J Am Soc Nephrol. 2016. PMID: 26620094 Free PMC article. No abstract available.
References
-
- Eddy AA, Symons JM: Nephrotic syndrome in childhood. Lancet 362: 629–639, 2003 - PubMed
-
- Gubler MC: Podocyte differentiation and hereditary proteinuria/nephrotic syndromes. J Am Soc Nephrol 14[Suppl 1]: S22–S26, 2003 - PubMed
-
- Lombel RM, Gipson DS, Hodson EM Kidney Disease: Improving Global Outcomes : Treatment of steroid-sensitive nephrotic syndrome: New guidelines from KDIGO. Pediatr Nephrol 28: 415–426, 2013 - PubMed
-
- Coiffier B: Rituximab therapy in malignant lymphoma. Oncogene 26: 3603–3613, 2007 - PubMed
-
- Boumans MJ, Thurlings RM, Yeo L, Scheel-Toellner D, Vos K, Gerlag DM, Tak PP: Rituximab abrogates joint destruction in rheumatoid arthritis by inhibiting osteoclastogenesis. Ann Rheum Dis 71: 108–113, 2012 - PubMed
Publication types
MeSH terms
Substances
Supplementary concepts
LinkOut - more resources
Full Text Sources
Other Literature Sources
Research Materials
