

Healthcare decision-making in end stage renal disease-patient preferences and clinical correlates
- PMID: 26572607
- PMCID: PMC4647276
- DOI: 10.1186/s12882-015-0180-8
Healthcare decision-making in end stage renal disease-patient preferences and clinical correlates
Abstract
Background: Medical decision-making is critical to patient survival and well-being. Patients with end stage renal disease (ESRD) are faced with incrementally complex decision-making throughout their treatment journey. The extent to which patients seek involvement in the decision-making process and factors which influence these in ESRD need to be understood.
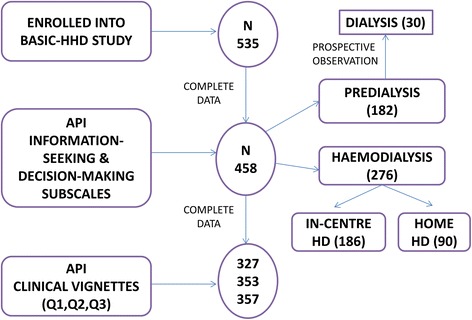
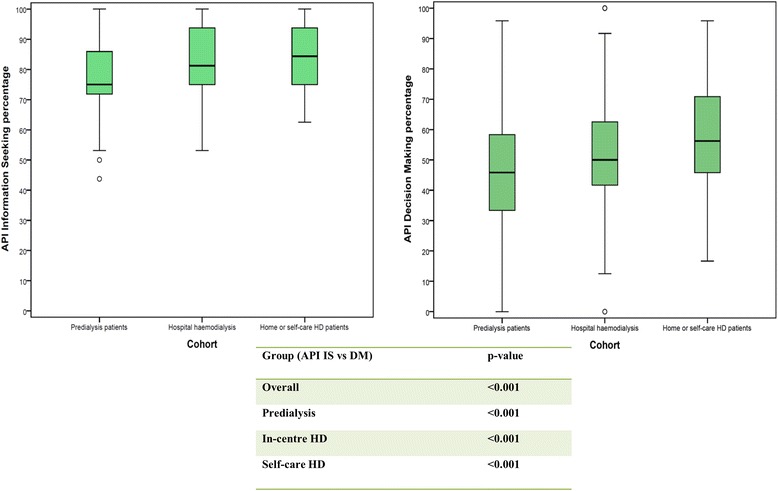
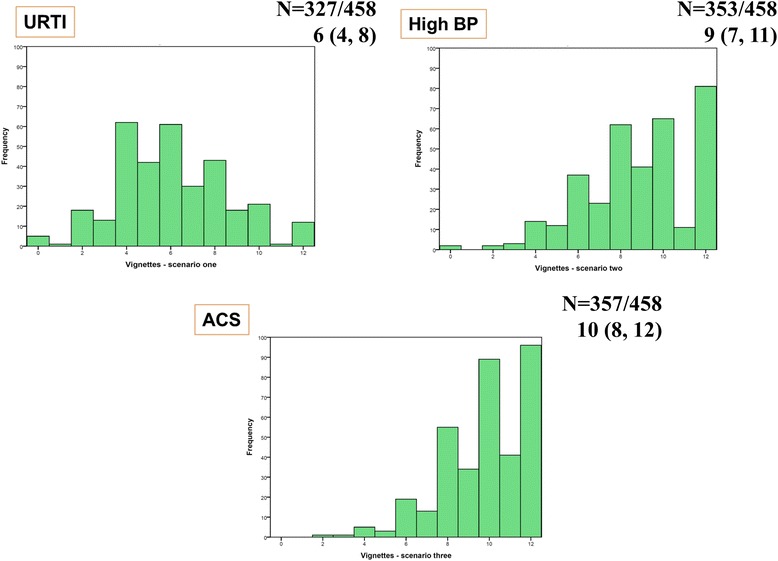
Methods: 535 ESRD patients were enrolled into the cross-sectional study arm and 30 patients who started dialysis were prospectively evaluated. Patients were enrolled into 3 groups- 'predialysis' (group A), 'in-centre' haemodialysis (HD) (group B) and self-care HD (93 % at home-group C) from across five tertiary UK renal centres. The Autonomy Preference Index (API) has been employed to study patient preferences for information-seeking (IS) and decision-making (DM). Demographic, psychosocial and neuropsychometric assessments are considered for analyses.
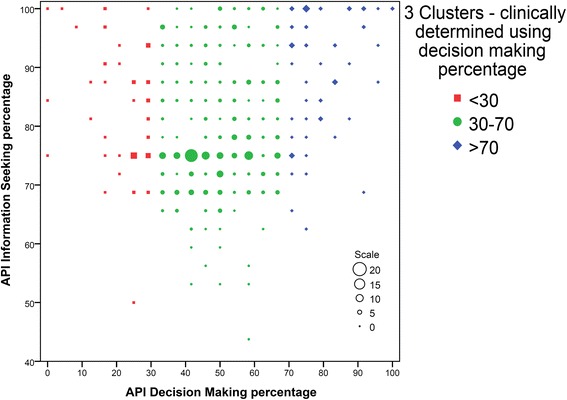
Results: 458 complete responses were available. API items have high internal consistency in the study population (Cronbach's alpha > 0.70). Overall and across individual study groups, the scores for information-seeking and decision-making are significantly different indicating that although patients had a strong preference to be well informed, they were more neutral in their preference to participate in DM (p < 0.05). In the age, education and study group adjusted multiple linear regression analysis, lower age, female gender, marital status; higher API IS scores and white ethnicity background were significant predictors of preference for decision-making. DM scores were subdivided into tertiles to identify variables associated with high (DM > 70: and low DM (≤30) scores. This shows association of higher DM scores with lower age, lower comorbidity index score, higher executive brain function, belonging in the self-caring cohort and being unemployed. In the prospectively studied cohort of predialysis patients, there was no change in decision-making preference scores after commencement of dialysis.
Conclusion: ESRD patients prefer to receive information, but this does not always imply active involvement in decision-making. By understanding modifiable and non-modifiable factors which affect patient preferences for involvement in healthcare decision-making, health professionals may acknowledge the need to accommodate individual patient preferences to the extent determined by the individual patient factors.
Figures
Similar articles
-
What influences patient choice of treatment modality at the pre-dialysis stage?Nephrol Dial Transplant. 2012 Apr;27(4):1542-7. doi: 10.1093/ndt/gfr452. Epub 2011 Aug 23. Nephrol Dial Transplant. 2012. PMID: 21865216 Clinical Trial.
-
Conflict when making decisions about dialysis modality.J Clin Nurs. 2018 Jan;27(1-2):e138-e146. doi: 10.1111/jocn.13890. Epub 2017 Jul 17. J Clin Nurs. 2018. PMID: 28543737
-
Veterans' decision-making preferences and perceived involvement in care for chronic heart failure.Heart Lung. 2008 Nov-Dec;37(6):440-8. doi: 10.1016/j.hrtlng.2008.02.003. Epub 2008 Sep 30. Heart Lung. 2008. PMID: 18992627
-
Patients' preference for involvement in medical decision making: a narrative review.Patient Educ Couns. 2006 Feb;60(2):102-14. doi: 10.1016/j.pec.2005.02.003. Patient Educ Couns. 2006. PMID: 16442453 Review.
-
Collaborative end-of-life decision making in end stage renal disease.ANNA J. 1998 Dec;25(6):615-7, 597. ANNA J. 1998. PMID: 10188397 Review.
Cited by
-
When attitudes and beliefs get in the way of shared decision-making: A mediation analysis of participation preference.Health Expect. 2023 Apr;26(2):740-751. doi: 10.1111/hex.13699. Epub 2023 Jan 13. Health Expect. 2023. PMID: 36639880 Free PMC article.
-
The Burden of Cognitive Impairment in Patients With End-Stage Renal Disease and Impact on Dialysis Modality Choice.Kidney Int Rep. 2016 Aug 10;1(4):240-249. doi: 10.1016/j.ekir.2016.07.010. eCollection 2016 Nov. Kidney Int Rep. 2016. PMID: 29142928 Free PMC article.
-
Factors promoting shared decision-making in renal replacement therapy for patients with end-stage kidney disease: systematic review and qualitative meta-synthesis.Int Urol Nephrol. 2022 Mar;54(3):553-574. doi: 10.1007/s11255-021-02913-8. Epub 2021 Jun 22. Int Urol Nephrol. 2022. PMID: 34159522 Free PMC article.
-
Healthcare professional education in shared decision making in the context of chronic kidney disease: a scoping review.BMC Nephrol. 2023 Jun 29;24(1):195. doi: 10.1186/s12882-023-03229-8. BMC Nephrol. 2023. PMID: 37386464 Free PMC article.
-
Decision-making for people with dementia and advanced kidney disease: a secondary qualitative analysis of interviews from the Conservative Kidney Management Assessment of Practice Patterns Study.BMJ Open. 2018 Nov 12;8(11):e022385. doi: 10.1136/bmjopen-2018-022385. BMJ Open. 2018. PMID: 30420346 Free PMC article.
References
-
- Tan TZ, Ng GS, Quek C. A Decision Making System Based on Complementary Learning. Intell Syst Ref Libr. 2010;4:163–179. doi: 10.1007/978-3-642-13639-9_7. - DOI
-
- A. Coulter and A. Collins, “MAKING DECISION-MAKING A REALITY No decision about me, without me,” Kings Fund, pp. 1–56, 2011.
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
