

Role of KRAS-LCS6 polymorphism in advanced NSCLC patients treated with erlotinib or docetaxel in second line treatment (TAILOR)
- PMID: 26573509
- PMCID: PMC4648064
- DOI: 10.1038/srep16331
Role of KRAS-LCS6 polymorphism in advanced NSCLC patients treated with erlotinib or docetaxel in second line treatment (TAILOR)
Abstract
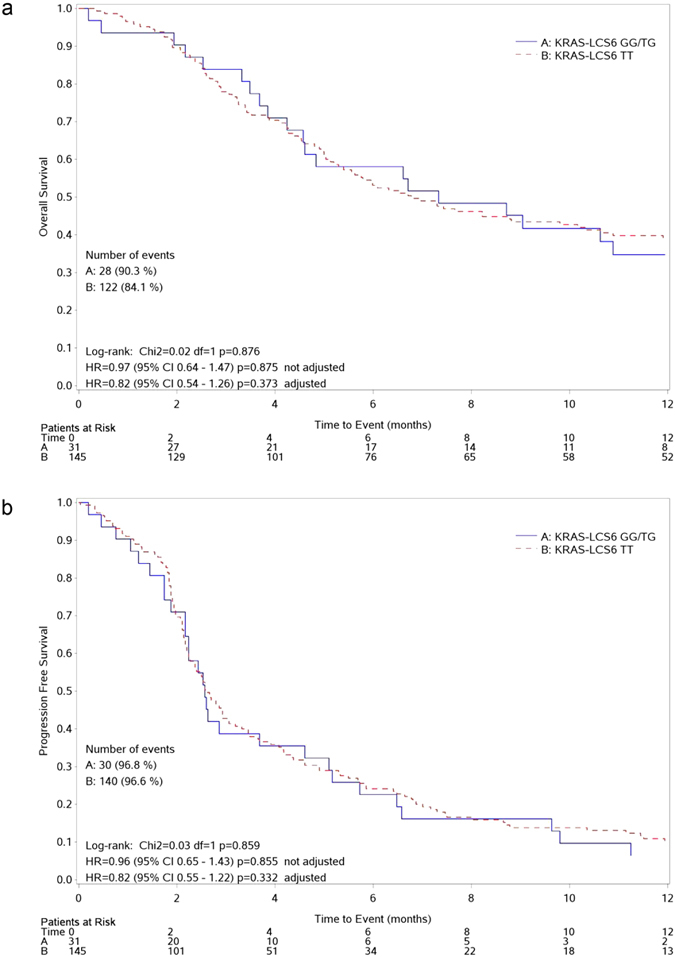
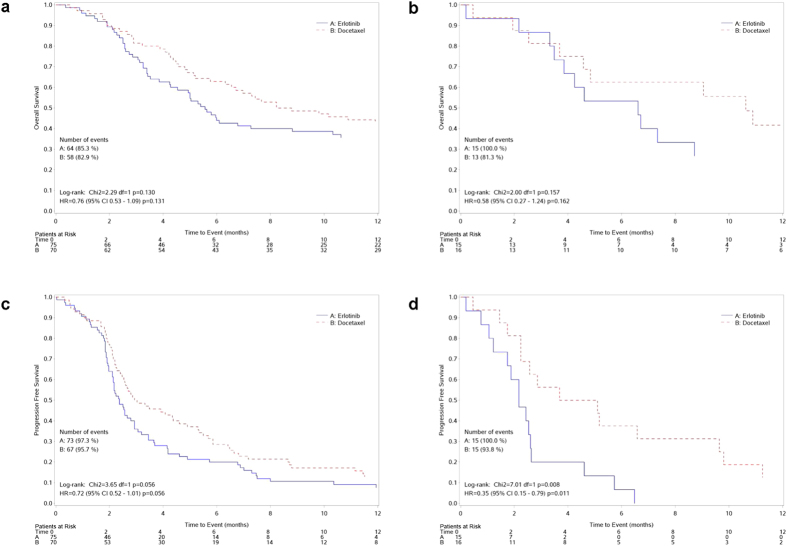
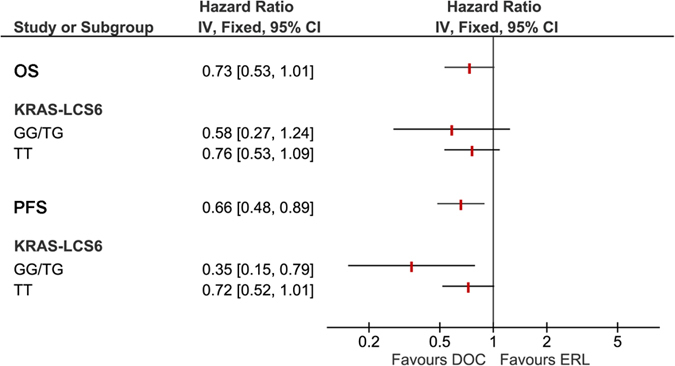
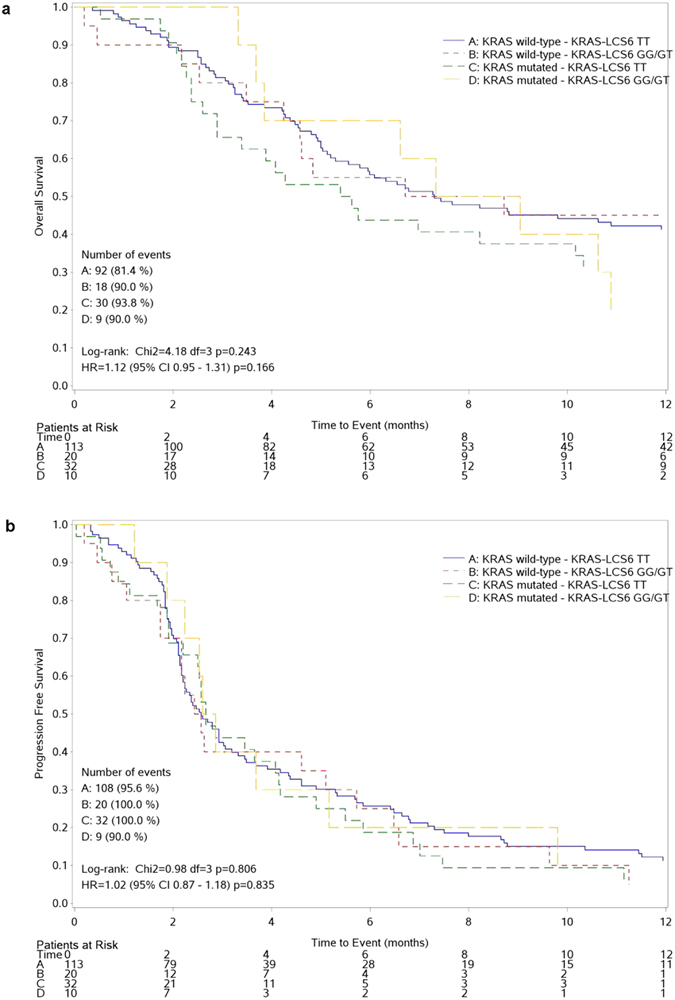
MicroRNAs were described to target mRNA and regulate the transcription of genes involved in processes de-regulated in tumorigenesis, such as proliferation, differentiation and survival. In particular, the miRNA let-7 has been suggested to regulate the expression of the KRAS gene, a common mutated gene in non-small cell lung cancer (NSCLC), through a let-7 complementary site (LCS) in 3'UTR of KRAS mRNA. We have reported the analysis performed on the role of the polymorphism located in the KRAS-LCS (rs61764370) which is involved in the disruption of the let-7 complementary site in NSCLC patients enrolled within the TAILOR trial, a randomised trial comparing erlotinib versus docetaxel in second line treatment. In our cohort of patients, KRAS-LCS6 polymorphism did not have any impact on both overall survival (OS) and progression free survival (PFS) and was not associated with any patient's baseline characteristics included in the study. Overall, patients had a better prognosis when treated with docetaxel instead of erlotinib for both OS and PFS. Considering KRAS-LCS6 status, the TG/GG patients had a benefit from docetaxel treatment (HR(docetaxel vs erlotinib) = 0.35, 95% CI 0.15-0.79, p = 0.011) compared with the TT patients (HR(docetaxel vs erlotinib) = 0.72, 95% CI 0.52-1.01, p = 0.056) in terms of PFS.
Figures
References
-
- Jemal A. et al. Global cancer statistics. CA Cancer J Clin 61, 69–90 (2011). - PubMed
-
- Sato M., Shames D. S., Gazdar A. F. & Minna J. D. A translational view of the molecular pathogenesis of lung cancer. J Thorac Oncol 2, 327–343 (2007). - PubMed
-
- Riely G. J., Marks J. & Pao W. KRAS mutations in non-small cell lung cancer. Proc Am Thorac Soc 6, 201–205 (2009). - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Miscellaneous
