

Personalizing blood pressure management in septic shock
- PMID: 26573630
- PMCID: PMC4646890
- DOI: 10.1186/s13613-015-0085-5
Personalizing blood pressure management in septic shock
Abstract
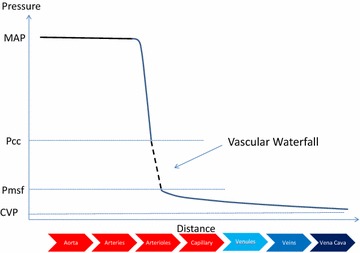
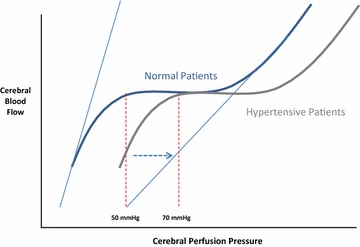
This review examines the available evidence for targeting a specific mean arterial pressure (MAP) in sepsis resuscitation. The clinical data suggest that targeting an MAP of 65-70 mmHg in patients with septic shock who do not have chronic hypertension is a reasonable first approximation. Whereas in patients with chronic hypertension, targeting a higher MAP of 80-85 mmHg minimizes renal injury, but it comes with increased risk of arrhythmias. Importantly, MAP alone should not be used as a surrogate of organ perfusion pressure, especially under conditions in which intracranial, intra-abdominal or tissue pressures may be elevated. Organ-specific perfusion pressure targets include 50-70 mmHg for the brain based on trauma brain injury as a surrogate for sepsis, 65 mmHg for renal perfusion and >50 mmHg for hepato-splanchnic flow. Even at the same MAP, organs and regions within organs may have different perfusion pressure and pressure-flow relationships. Thus, once this initial MAP target is achieved, MAP should be titrated up or down based on the measures of organ function and tissue perfusion.
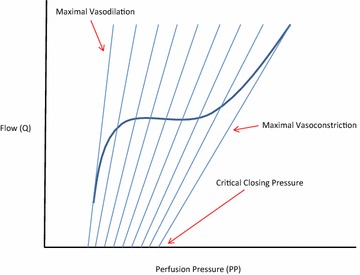
Keywords: Arterial blood pressure; Autoregulation; Critical closing pressure; Organ blood flow; Resuscitation; Sepsis; Septic shock; Vasopressor therapy.
Figures
References
LinkOut - more resources
Full Text Sources
Other Literature Sources
