

Effects of adding Braun jejunojejunostomy to standard Whipple procedure on reduction of afferent loop syndrome - a randomized clinical trial
- PMID: 26574829
- PMCID: PMC4651689
- DOI: 10.1503/cjs.005215
Effects of adding Braun jejunojejunostomy to standard Whipple procedure on reduction of afferent loop syndrome - a randomized clinical trial
Abstract
Background: Whipple surgery (pancreaticodeudenectomy) has a high complication rate. We aimed to evaluate whether adding Braun jejunojejunostomy (side-to-side anastomosis of afferent and efferent loops distal to the gastrojejunostomy site) to a standard Whipple procedure would reduce postoperative complications.
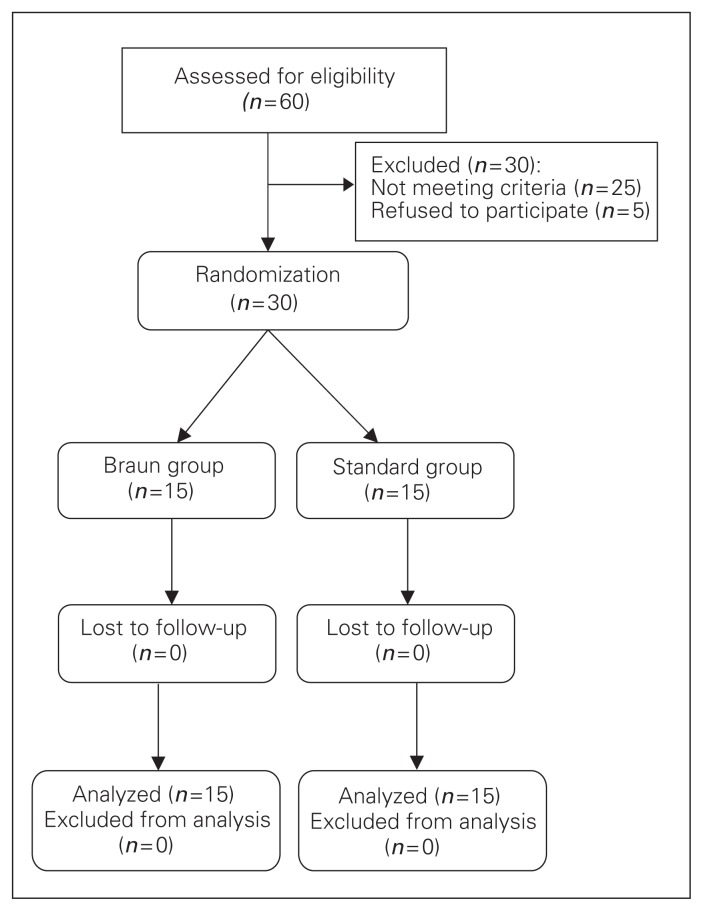
Methods: We conducted a randomized clinical trial comparing patients who underwent standard Whipple surgery (standard group) and patients who underwent standard Whipple surgery with Braun jejunojejunostomy (Braun group). Patients were followed for 1 month after the procedure and postoperative complications were recorded.
Results: Our study included 30 patients: 15 in the Braun and 15 in the standard group. In the Braun group, 4 (26.7%) patients experienced 6 complications, whereas in the standard group, 7 (46.7%) patients experienced 11 complications (p = 0.14). Complications in the Braun group were gastrointestinal bleeding and wound infection (n = 1 each) and delayed gastric emptying and pulmonary infection (n = 2 each). Complications in the standard group were death, pancreatic anastomosis leak and biliary anastomosis leak (n = 1 each); gastrointestinal bleeding (n = 2); and afferent loop syndrome and delayed gastric emptying (n = 3 each). There was no significant difference between groups in the subtypes of complications.
Conclusion: Our results showed that adding Braun jejunojejunostomy to standard Whipple procedure was associated with lower rates of afferent loop syndrome and delayed gastric emptying. However, more studies are needed to define the role of Braun jejunojejunostomy in this regard.
Trial registration: IRCT2014020316473N1 (www.irct.ir).
Contexte: La chirurgie de Whipple (pancréatoduodénectomie) s’accompagne de taux de complications élevés. Nous avons voulu vérifier si l’ajout d’une jéjunojéjunostomie de Braun (anastomose latérolatérale des anses afférente et efférente à la partie distale de la gastrojéjunostomie) à une chirurgie de Whipple standard permet de réduire les complications postopératoires.
Méthodes: Nous avons procédé à un essai clinique randomisé pour comparer des patients soumis à une chirurgie de Whipple standard (groupe standard) à des patients soumis à une chirugie de Whipple standard avec jéjunojéjunostomie de Braun (groupe Braun). Les patients ont été suivis pendant 1 mois après l’intervention et les complications postopératoires ont été notées.
Résultats: Notre étude a regroupé 30 patients : 15 dans le groupe Braun et 15 dans le groupe standard. Dans le groupe Braun, 4 patients (26,7 %) ont présenté 6 complications, tandis que dans le groupe standard, 7 patients (46,7 %) ont présenté 11 complications (p = 0,14). Les complications dans le groupe Braun ont été saignements gastro- intestinaux et infection de plaie (n = 1 chacun) et retard de la vidange gastrique et infection pulmonaire (n = 2 chacun). Les complications dans le groupe standard ont été décès, fuite de l’anastomose pancréatique et fuite de l’anastomose biliaire (n = 1 chacun); saignement gastro- intestinal (n = 2); et syndrome de l’anse afférente et retard de la vidange gastrique (n = 3 chacun). On n’a noté aucune différence significative entre les groupes pour ce qui est des sous-types de complications.
Conclusion: Nos résultats ont montré que l’ajout de la jéjunojéjunostomie de Braun à une chirurgie de Whipple standard a été associé à des taux moindres de syndrome de l’anse afférente et de retard de la vidange gastrique. Il faudra toutefois procéder à d’autres études pour définir le rôle de la jéjunojéjunostomie de Braun à cet égard.
Enregistrement de l’essai: IRCT2014020316473N1 (www.irct.ir).
Similar articles
-
Braun anastomosis lowers the incidence of delayed gastric emptying following pancreaticoduodenectomy: a meta-analysis.BMC Gastroenterol. 2018 Nov 26;18(1):176. doi: 10.1186/s12876-018-0909-5. BMC Gastroenterol. 2018. PMID: 30477442 Free PMC article.
-
Impact of Braun anastomosis on reducing delayed gastric emptying following pancreaticoduodenectomy: a prospective, randomized controlled trial.J Hepatobiliary Pancreat Sci. 2016 Jun;23(6):364-72. doi: 10.1002/jhbp.349. Epub 2016 Apr 24. J Hepatobiliary Pancreat Sci. 2016. PMID: 27038406 Clinical Trial.
-
Acute afferent loop syndrome in the early postoperative period following pancreaticoduodenectomy.Ann R Coll Surg Engl. 2015 Jul;97(5):349-53. doi: 10.1308/003588414X14055925061036. Ann R Coll Surg Engl. 2015. PMID: 26264085 Free PMC article.
-
Efficacy of Endoscopically Created Bypass Anastomosis in Treatment of Afferent Limb Syndrome: A Single-Center Study.Clin Gastroenterol Hepatol. 2016 Apr;14(4):633-7. doi: 10.1016/j.cgh.2015.11.010. Epub 2015 Dec 7. Clin Gastroenterol Hepatol. 2016. PMID: 26674590
-
Therapeutic strategies for the management of delayed gastric emptying after pancreatic resection.Langenbecks Arch Surg. 2007 Jan;392(1):1-12. doi: 10.1007/s00423-006-0096-7. Epub 2006 Oct 5. Langenbecks Arch Surg. 2007. PMID: 17021788 Review.
Cited by
-
EUS-guided gastrojejunostomy with an esophageal fully covered self-expanding metal stent for the management of benign afferent loop obstruction.VideoGIE. 2018 Jun 12;3(7):213-216. doi: 10.1016/j.vgie.2018.04.007. eCollection 2018 Jul. VideoGIE. 2018. PMID: 30128393 Free PMC article. No abstract available.
-
Outcome of endoscopic small-bore naso-jejunal tube stenting in early postoperative jejunal limb obstruction after gastrectomy.Surg Endosc. 2019 Feb;33(2):520-527. doi: 10.1007/s00464-018-6326-6. Epub 2018 Jul 12. Surg Endosc. 2019. PMID: 30003345
-
Reduction of pancreatic anastomotic leakage after pancreaticoduodenectomy.Can J Surg. 2018 Apr;61(2):E3. doi: 10.1503/cjs.1861021. Can J Surg. 2018. PMID: 29582752 Free PMC article. No abstract available.
-
Braun anastomosis lowers the incidence of delayed gastric emptying following pancreaticoduodenectomy: a meta-analysis.BMC Gastroenterol. 2018 Nov 26;18(1):176. doi: 10.1186/s12876-018-0909-5. BMC Gastroenterol. 2018. PMID: 30477442 Free PMC article.
-
Treatment strategies to prevent or mitigate the outcome of postpancreatectomy hemorrhage: a review of randomized trials.Int J Surg. 2024 Oct 1;110(10):6145-6154. doi: 10.1097/JS9.0000000000000876. Int J Surg. 2024. PMID: 37983766 Free PMC article.
References
-
- Büchler MW, Wagner M, Schmied BM, et al. Changes in mortality after pancreatic resection: towards the end of completion pancreatectomy. Arch Surg. 2003;138:1310–4. - PubMed
-
- Balcom JH, Rattner DW, Warshaw AL, et al. Ten-year experience with 733 pancreatic resections: changing indications, older patients, and decreasing length of hospitalization. Arch Surg. 2001;136:391–8. - PubMed
-
- Sohn TA, Campbell KA, Pitt HA, et al. Quality of life and long-term survival after surgery for chronic pancreatitis. J Gastrointest Surg. 2000;4:355–65. - PubMed
-
- Shimoda M, Kubota K, Katoh M, et al. Effect of Billroth II or Roux-en-Y reconstruction for the gastrojejunostomy on delayed gastric emptying after pancreaticoduodenectomy: a randomized controlled study. Ann Surg. 2013;257:938–42. - PubMed
Publication types
MeSH terms
Associated data
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical