

Early experience with robotic pancreatic surgery in a Canadian institution
- PMID: 26574831
- PMCID: PMC4651691
- DOI: 10.1503/cjs.003815
Early experience with robotic pancreatic surgery in a Canadian institution
Abstract
Background: Pancreatic resections have traditionally been associated with substantial morbidity and mortality. The robotic platform is believed to improve technical aspects of the procedure while offering minimally invasive benefits. We sought to determine the safety and feasibility of the first robotic pancreaticoduodenectomies performed at our institution.
Methods: We retrospectively reviewed data on all patients who underwent robotic-assisted pancreaticoduodenectomy (RAPD) between July 2010 and June 2014 and compared them to outcomes of patients undergoing hybrid laparoscopic pancreaticoduodenectomies (HLAPD) during the same time period.
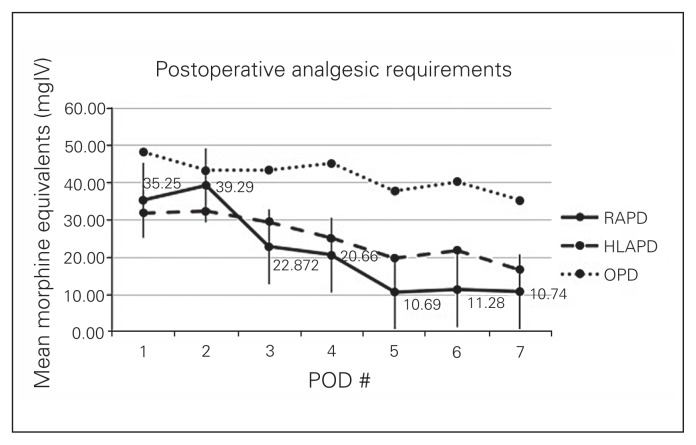
Results: Fifteen patients were scheduled for RAPD; 2 were converted to an open approach and 1 to a mini-laparotomy during the laparoscopic portion of the procedure. Patients who had RAPD (n = 12) had a median duration of surgery of 596.6 (range 509-799) minutes, estimated blood loss of 275 (range 50-1000) mL and median length of stay of 7.5 (range 5-57) days. Mean total opioid use up to postoperative day 7 was 142.599 ± 68.2 versus 176.9 ± 112.7 mg equivalents of intravenous morphine for RAPD and HLAPD, respectively. There was no significant difference between RAPD and HLAPD in any parameters, highlighting the safety and feasibility of a step-wise minimally invasive learning platform. Most patients in the RAPD group had malignant pathology (88.2%). Oncologic outcomes were maintained with no significant difference in ability to resect lymph nodes or achieve negative margins. There were 4 (28.5%) Clavien I-II complications and 3 (29.4%) Clavien III- IV complications, 2 of which required readmission. There were no reported deaths at 90 days. Complication, pancreatic leak and mortality rates did not differ significantly from our laparoscopic experience.
Conclusion: Outcomes of RAPD and HLAPD were comparable at our centre, even during the early stages of our learning curve. These results also highlight the safety, feasibility and patient benefits of a step-wise transition from open to hybrid to fully robotic pancreaticoduodenectomies in a high-volume academic centre.
Contexte: L’ablation du pancréas a de tout temps été associée à une morbidité et une mortalité importantes. Le recours à une plateforme assistée par robot devrait vraisemblablement améliorer les aspects techniques de l’intervention et offrir en même temps les avantages d’une intervention minimalement effractive. Nous avons voulu déterminer l’innocuité et la faisabilité des premières pancréatoduodénectomies assistées par robot effectuées dans notre établissement.
Méthodes: Nous avons passé en revue de manière rétrospective les données concernant tous les patients ayant subi une pancréatoduodénectomie assistée par robot (PDAR) entre juillet 2010 et juin 2014 et nous les avons comparées aux résultats enregistrés chez les patients ayant subi une pancréatoduodénectomie laparoscopique hybride (PDLH) au cours de la même période.
Résultats: Quinze patients ont été pressentis pour une PDAR; 2 ont plutôt subi une intervention ouverte et 1 a subi une mini-laparotomie durant la portion laparoscopique de l’intervention. Chez les patients soumis à la PDAR (n = 12), la durée médiane de la chirurgie a été de 596,6 (plage de 509 à 799) minutes, les pertes sanguines estimées ont été de 275 (plage de 50 à 1000) mL et la durée médiane du séjour hospitalier a été de 7,5 (plage de 5 à 57) jours. L’utilisation totale moyenne d’opioïdes jusqu’au septième jour postopératoire a été de 142,599 ± 68,2 mg équivalents de morphine intraveineuse contre 176,9 ± 112,7 pour la PDAR et la PDLH, respectivement. On n’a noté aucune différence significative entre la PDAR et la PDLH au plan des paramètres, ce qui souligne l’innocuité et la faisabilité d’une plateforme d’apprentissage séquentielle minimalement effractive. La plupart des patients du groupe soumis à la PDAR étaient atteints d’un cancer (88,2 %). Les paramètres oncologiques se sont maintenus, sans différence significative quant à la capacité de réséquer les ganglions lymphatiques ou d’obtenir des marges négatives. On a dénombré 4 (28,5 %) complications de stade I–II et 3 (29,4 %) de stade III–IV selon la classification de Clavien; 2 de ces dernières ont nécessité une réadmission. On n’a déploré aucun décès à 90 jours. Les taux de complications, de fuite pancréatique et de mortalité n’ont pas différé significativement par rapport à nos interventions laparoscopiques.
Conclusion: Les résultats de la PDAR et de la PDLH ont été comparables dans notre établissement, même aux premières étapes de notre courbe d’apprentissage. De tels résultats soulignent l’innocuité, la faisabilité et les bienfaits pour les patients d’une transition graduelle des pancréatoduodénectomies ouvertes, hybrides puis entièrement assistées par robot dans un centre universitaire traitant de forts volumes de patients.
Figures
References
-
- Giulianotti PC, Sbrana F, Bianco FM, et al. Robot-assisted laparoscopic pancreatic surgery: single-surgeon experience. Surg Endosc. 2010;24:1646–57. - PubMed
-
- Correa-Gallego C, Dinkelspiel HE, Sulimanoff I, et al. Minimally-invasive vs open pancreaticoduodenectomy: systematic review and meta-analysis. J Am Coll Surg. 2014;218:129–39. - PubMed
-
- Lei P, Wei B, Guo W, et al. Minimally invasive surgical approach compared with open pancreaticoduodenectomy: a systematic review and meta-analysis on the feasibility and safety. Surg Laparosc Endosc Percutan Tech. 2014;24:296–305. - PubMed
-
- Giulianotti PC, Coratti A, Angelini M, et al. Robotics in general surgery: personal experience in a large community hospital. Arch surg. 2003;138:777–84. - PubMed
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical