

Early Administration of Azithromycin and Prevention of Severe Lower Respiratory Tract Illnesses in Preschool Children With a History of Such Illnesses: A Randomized Clinical Trial
- PMID: 26575060
- PMCID: PMC4757487
- DOI: 10.1001/jama.2015.13896
Early Administration of Azithromycin and Prevention of Severe Lower Respiratory Tract Illnesses in Preschool Children With a History of Such Illnesses: A Randomized Clinical Trial
Erratum in
-
Error in the Figure.JAMA. 2016 Jan 12;315(2):204. doi: 10.1001/jama.2015.17376. JAMA. 2016. PMID: 26757476 No abstract available.
-
Error in the Text.JAMA. 2016 Jan 26;315(4):419. doi: 10.1001/jama.2015.17383. JAMA. 2016. PMID: 26813223 No abstract available.
Abstract
Importance: Many preschool children develop recurrent, severe episodes of lower respiratory tract illness (LRTI). Although viral infections are often present, bacteria may also contribute to illness pathogenesis. Strategies that effectively attenuate such episodes are needed.
Objective: To evaluate if early administration of azithromycin, started prior to the onset of severe LRTI symptoms, in preschool children with recurrent severe LRTIs can prevent the progression of these episodes.
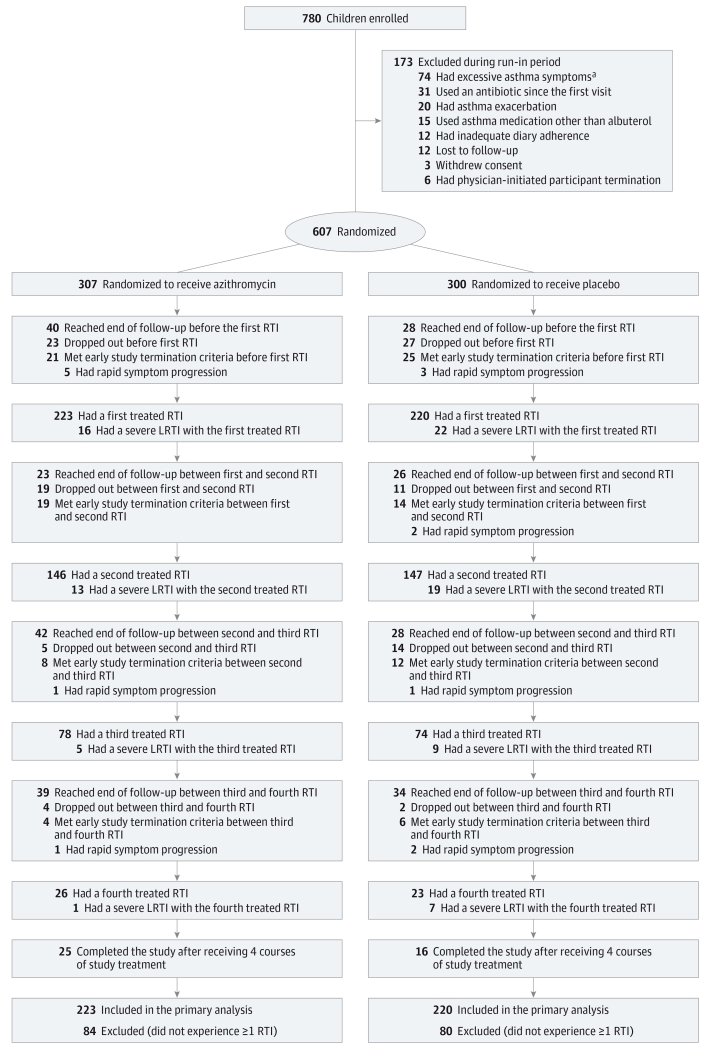
Design, setting, and participants: A randomized, double-blind, placebo-controlled, parallel-group trial conducted across 9 academic US medical centers in the National Heart, Lung, and Blood Institute's AsthmaNet network, with enrollment starting in April 2011 and follow-up complete by December 2014. Participants were 607 children aged 12 through 71 months with histories of recurrent, severe LRTIs and minimal day-to-day impairment.
Intervention: Participants were randomly assigned to receive azithromycin (12 mg/kg/d for 5 days; n = 307) or matching placebo (n = 300), started early during each predefined RTI (child's signs or symptoms prior to development of LRTI), based on individualized action plans, over a 12- through 18-month period.
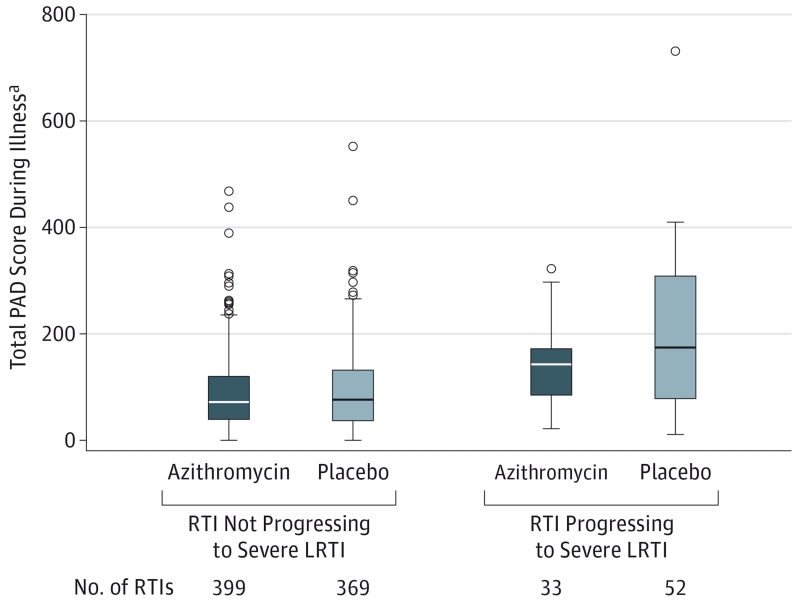
Main outcomes and measures: The primary outcome measure was the number of RTIs not progressing to a severe LRTI, measured at the level of the RTI, that would in clinical practice trigger the prescription of oral corticosteroids. Presence of azithromycin-resistant organisms in oropharyngeal samples, along with adverse events, were among the secondary outcome measures.
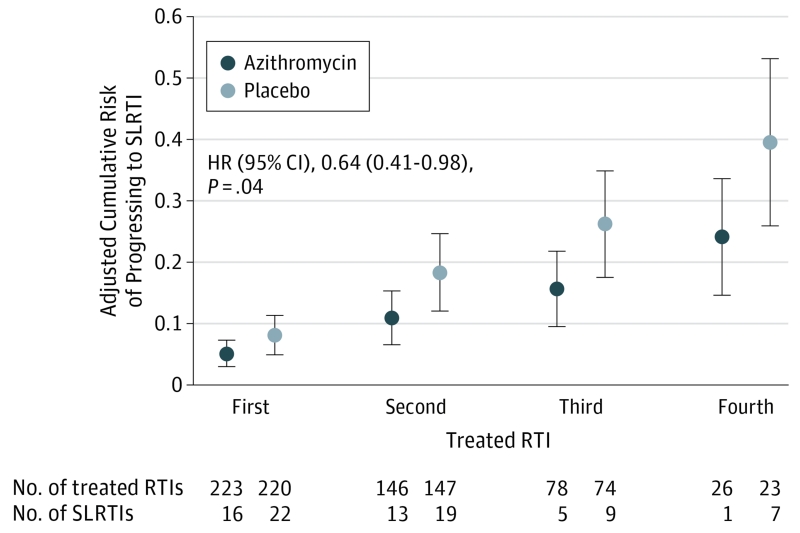
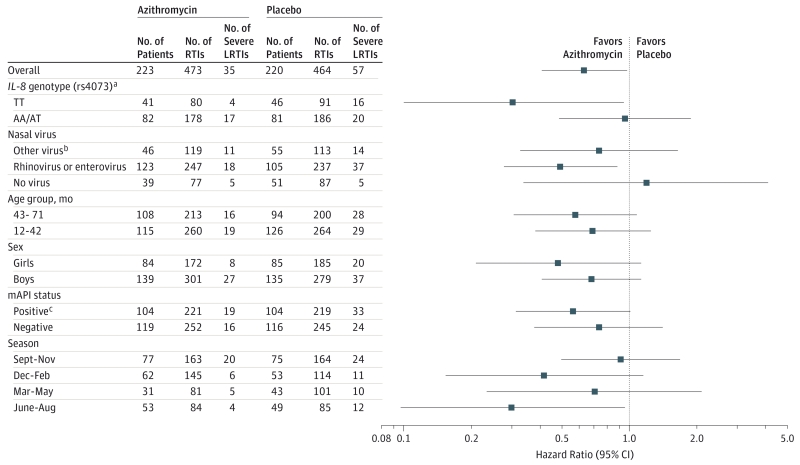
Results: A total of 937 treated RTIs (azithromycin group, 473; placebo group, 464) were experienced by 443 children (azithromycin group, 223; placebo group, 220), including 92 severe LRTIs (azithromycin group, 35; placebo group, 57). Azithromycin significantly reduced the risk of progressing to severe LRTI relative to placebo (hazard ratio, 0.64 [95% CI, 0.41-0.98], P = .04; absolute risk for first RTI: 0.05 for azithromycin, 0.08 for placebo; risk difference, 0.03 [95% CI, 0.00-0.06]). Induction of azithromycin-resistant organisms and adverse events were infrequently observed.
Conclusions and relevance: Among young children with histories of recurrent severe LRTIs, the use of azithromycin early during an apparent RTI compared with placebo reduced the likelihood of severe LRTI. More information is needed on the development of antibiotic-resistant pathogens with this strategy.
Trial registration: clinicaltrials.gov Identifier: NCT01272635.
Figures
Comment in
-
[Exogenous harmful substances in pregnancy and their effects on the embryo and fetus].Zentralbl Gynakol. 1988;110(24):1546-55. Zentralbl Gynakol. 1988. PMID: 3066064 Review. German.
-
Individual Benefit vs Societal Effect of Antibiotic Prescribing for Preschool Children With Recurrent Wheeze.JAMA. 2015 Nov 17;314(19):2027-9. doi: 10.1001/jama.2015.14953. JAMA. 2015. PMID: 26575058 No abstract available.
-
Early use of azithromycin may reduce severity of wheezing, study finds.BMJ. 2015 Nov 18;351:h6153. doi: 10.1136/bmj.h6153. BMJ. 2015. PMID: 26582751 No abstract available.
-
Azithromycin may prevent severe respiratory-infection-induced wheezing.J Pediatr. 2016 May;172:224-7. doi: 10.1016/j.jpeds.2016.02.029. J Pediatr. 2016. PMID: 27112084 No abstract available.
-
Early Azithromycin Treatment to Prevent Severe Lower Respiratory Tract Illnesses in Children.JAMA. 2016 May 17;315(19):2121-2. doi: 10.1001/jama.2016.0918. JAMA. 2016. PMID: 27187308 Free PMC article. No abstract available.
-
Early Azithromycin Treatment to Prevent Severe Lower Respiratory Tract Illnesses in Children--Reply.JAMA. 2016 May 17;315(19):2122-3. doi: 10.1001/jama.2016.0921. JAMA. 2016. PMID: 27187309 No abstract available.
References
-
- Martinez FD, Wright AL, Taussig LM, Holberg CJ, Halonen M, Morgan WJ, The Group Health Medical Associates Asthma and wheezing in the first 6 years of life. N Engl J Med. 1995;332(3):133–138. - PubMed
-
- Ly NP, Gold DR, Weiss ST, Celedón JC. Recurrent wheeze in early childhood and asthma among children at risk for atopy. Pediatrics. 2006;117(6):e1132–e1138. - PubMed
-
- Moorman JE, Akinbami LJ, Bailey CM, et al. National surveillance of asthma: United States, 2001-2010. Vital Health Stat 3. 2012;(35):1–67. - PubMed
-
- Lemanske RF, Jr, Jackson DJ, Gangnon RE, et al. Rhinovirus illnesses during infancy predict subsequent childhood wheezing. J Allergy Clin Immunol. 2005;116(3):571–577. - PubMed
Publication types
MeSH terms
Substances
Associated data
Grants and funding
- HL098075/HL/NHLBI NIH HHS/United States
- U10 HL098107/HL/NHLBI NIH HHS/United States
- U10 HL098075/HL/NHLBI NIH HHS/United States
- K23 AI106945/AI/NIAID NIH HHS/United States
- U10 HL098096/HL/NHLBI NIH HHS/United States
- U10 HL098115/HL/NHLBI NIH HHS/United States
- HL098115/HL/NHLBI NIH HHS/United States
- HL098090/HL/NHLBI NIH HHS/United States
- TR000454/TR/NCATS NIH HHS/United States
- UL1 TR001082/TR/NCATS NIH HHS/United States
- HL098112/HL/NHLBI NIH HHS/United States
- TR000448/TR/NCATS NIH HHS/United States
- HL098107/HL/NHLBI NIH HHS/United States
- U10 HL064313/HL/NHLBI NIH HHS/United States
- HL098103/HL/NHLBI NIH HHS/United States
- K23 AI104780/AI/NIAID NIH HHS/United States
- UL1 TR001449/TR/NCATS NIH HHS/United States
- U10 HL098102/HL/NHLBI NIH HHS/United States
- U10 HL098177/HL/NHLBI NIH HHS/United States
- HL098098/HL/NHLBI NIH HHS/United States
- HL098102/HL/NHLBI NIH HHS/United States
- UL1 TR000439/TR/NCATS NIH HHS/United States
- TR001082/TR/NCATS NIH HHS/United States
- UL1 TR000454/TR/NCATS NIH HHS/United States
- U10 HL098103/HL/NHLBI NIH HHS/United States
- HL098177/HL/NHLBI NIH HHS/United States
- UL1 TR000041/TR/NCATS NIH HHS/United States
- UL1 TR000448/TR/NCATS NIH HHS/United States
- U10 HL098090/HL/NHLBI NIH HHS/United States
- U10 HL098112/HL/NHLBI NIH HHS/United States
- U10 HL098098/HL/NHLBI NIH HHS/United States
- TR000439/TR/NCATS NIH HHS/United States
- HL098096/HL/NHLBI NIH HHS/United States
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Miscellaneous
