

Botanical Drugs as an Emerging Strategy in Inflammatory Bowel Disease: A Review
- PMID: 26576073
- PMCID: PMC4630406
- DOI: 10.1155/2015/179616
Botanical Drugs as an Emerging Strategy in Inflammatory Bowel Disease: A Review
Abstract
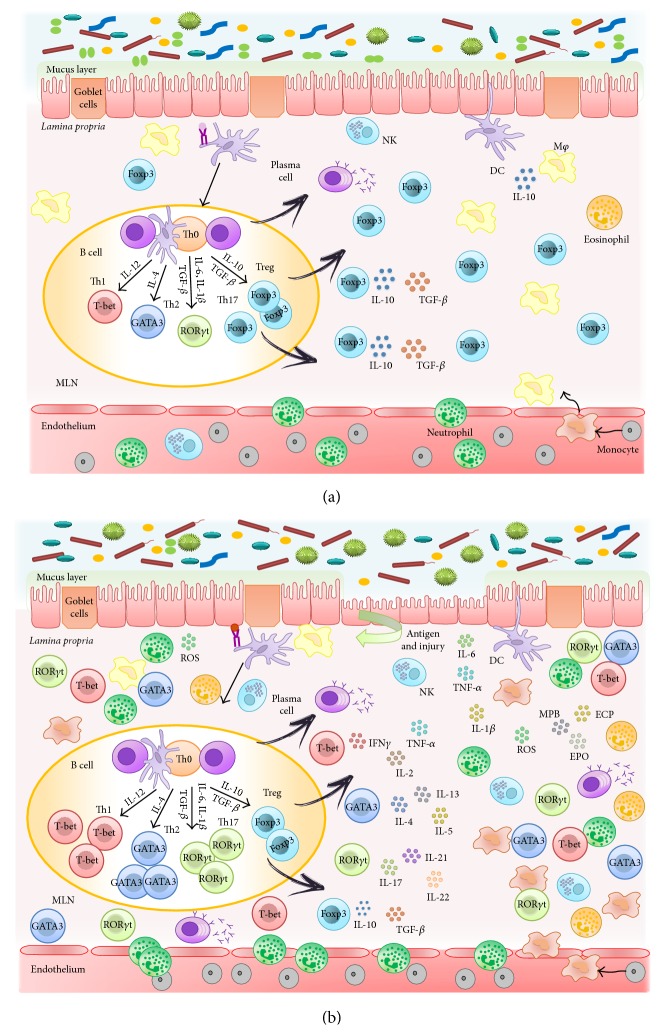
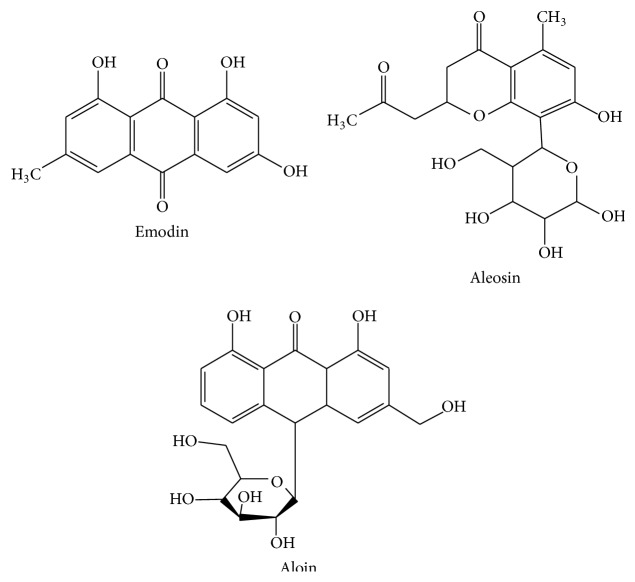
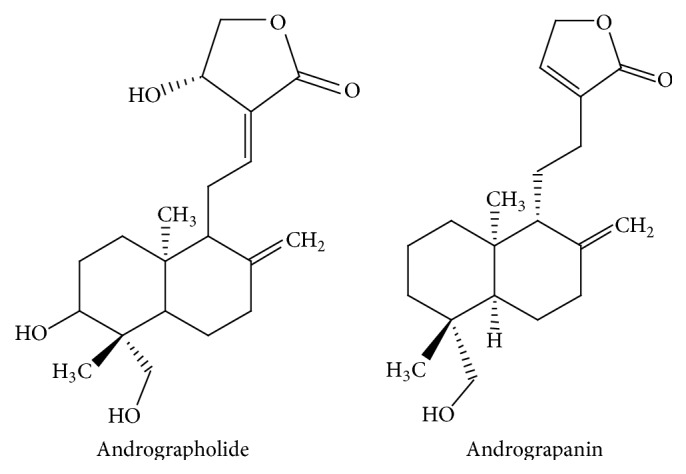
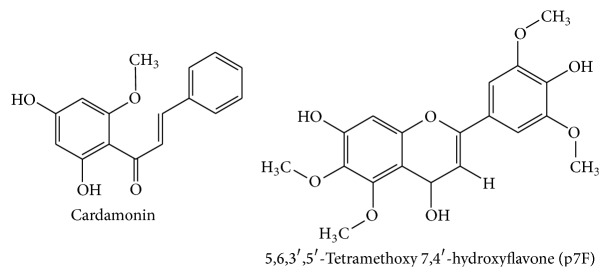
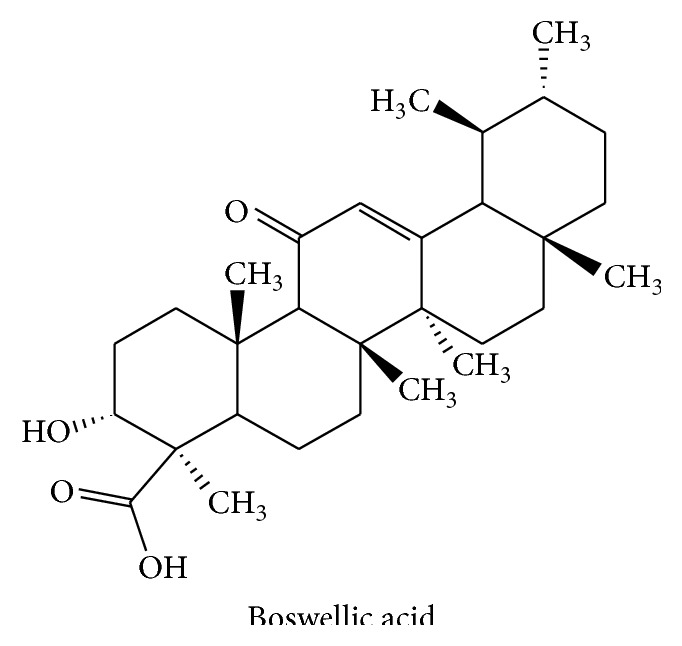
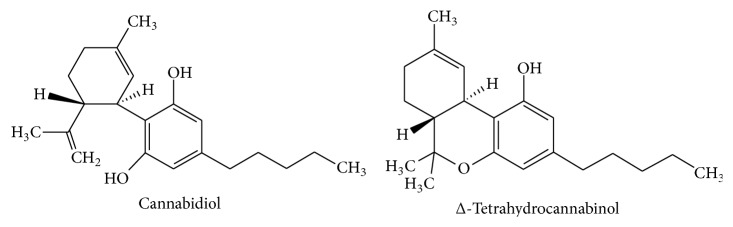
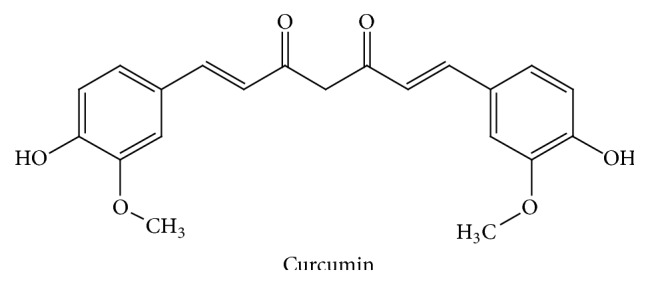
Crohn's disease and ulcerative colitis are the two most common categories of inflammatory bowel disease (IBD), which are characterized by chronic inflammation of the intestine that comprises the patients' life quality and requires sustained pharmacological and surgical treatments. Since their aetiology is not completely understood, nonfully efficient drugs have been developed and those that show effectiveness are not devoid of quite important adverse effects that impair their long-term use. Therefore, many patients try with some botanical drugs, which are safe and efficient after many years of use. However, it is necessary to properly evaluate these therapies to consider a new strategy for human IBD. In this report we have reviewed the main botanical drugs that have been assessed in clinical trials in human IBD and the mechanisms and the active compounds proposed for their beneficial effects.
Figures
Similar articles
-
Induction of clinical response and remission of inflammatory bowel disease by use of herbal medicines: a meta-analysis.World J Gastroenterol. 2013 Sep 14;19(34):5738-49. doi: 10.3748/wjg.v19.i34.5738. World J Gastroenterol. 2013. PMID: 24039370 Free PMC article.
-
Emerging Natural Therapies for the Treatment of Inflammatory Bowel Disease.Curr Pharm Biotechnol. 2025;26(8):1175-1188. doi: 10.2174/0113892010293150240415143650. Curr Pharm Biotechnol. 2025. PMID: 38716550 Review.
-
Dietary Supplement Therapies for Inflammatory Bowel Disease: Crohn's Disease and Ulcerative Colitis.Curr Pharm Des. 2016;22(2):180-8. doi: 10.2174/1381612822666151112145033. Curr Pharm Des. 2016. PMID: 26561079 Review.
-
Cannabis use amongst patients with inflammatory bowel disease.Eur J Gastroenterol Hepatol. 2011 Oct;23(10):891-6. doi: 10.1097/MEG.0b013e328349bb4c. Eur J Gastroenterol Hepatol. 2011. PMID: 21795981
-
Flavonoids in Inflammatory Bowel Disease: A Review.Nutrients. 2016 Apr 9;8(4):211. doi: 10.3390/nu8040211. Nutrients. 2016. PMID: 27070642 Free PMC article. Review.
Cited by
-
Cannabidiol Isolated From Cannabis sativa L. Protects Intestinal Barrier From In Vitro Inflammation and Oxidative Stress.Front Pharmacol. 2021 Apr 28;12:641210. doi: 10.3389/fphar.2021.641210. eCollection 2021. Front Pharmacol. 2021. PMID: 33995048 Free PMC article.
-
Flavonoids: structure-function and mechanisms of action and opportunities for drug development.Toxicol Res. 2021 Jan 20;37(2):147-162. doi: 10.1007/s43188-020-00080-z. eCollection 2021 Apr. Toxicol Res. 2021. PMID: 33868973 Free PMC article. Review.
-
Protective Effect of Amphipterygium adstringens Extract on Dextran Sulphate Sodium-Induced Ulcerative Colitis in Mice.Mediators Inflamm. 2016;2016:8543561. doi: 10.1155/2016/8543561. Epub 2016 Aug 21. Mediators Inflamm. 2016. PMID: 27635116 Free PMC article.
-
The Antioxidant Properties of Salvia verbenaca Extract Contribute to Its Intestinal Antiinflammatory Effects in Experimental Colitis in Rats.Antioxidants (Basel). 2023 Dec 2;12(12):2071. doi: 10.3390/antiox12122071. Antioxidants (Basel). 2023. PMID: 38136191 Free PMC article.
-
Endocannabinoid System as a Promising Therapeutic Target in Inflammatory Bowel Disease - A Systematic Review.Front Immunol. 2021 Dec 22;12:790803. doi: 10.3389/fimmu.2021.790803. eCollection 2021. Front Immunol. 2021. PMID: 35003109 Free PMC article.
References
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
