

Osseous vitality in single photon emission computed tomography/computed tomography (SPECT/CT) after balloon tibioplasty of the tibial plateau: a case series
- PMID: 26576635
- PMCID: PMC4650348
- DOI: 10.1186/s12880-015-0091-y
Osseous vitality in single photon emission computed tomography/computed tomography (SPECT/CT) after balloon tibioplasty of the tibial plateau: a case series
Abstract
Background: The minimally invasive, balloon-assisted reduction and cement-augmented internal fixation of the tibial plateau is an innovative surgical procedure for tibial plateau fractures. The close proximity of balloons and cement to the knee joint poses a potential risk for osteonecrosis; especially in the case of thin bone lamellae. However, there are no studies about the vitality of the cement-surrounding tissue after these tibioplasties. Therefore, our goal was to assess the osseous vitality after cement-augmented balloon tibioplasty using single photon emission computed tomography/computed tomography (SPECT/CT) in a series of patients.
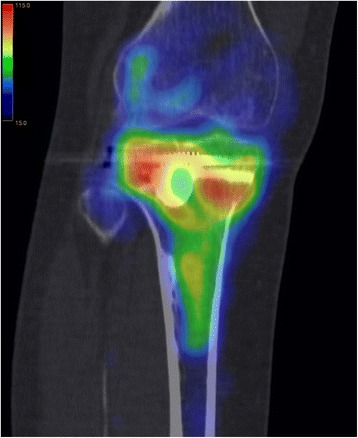
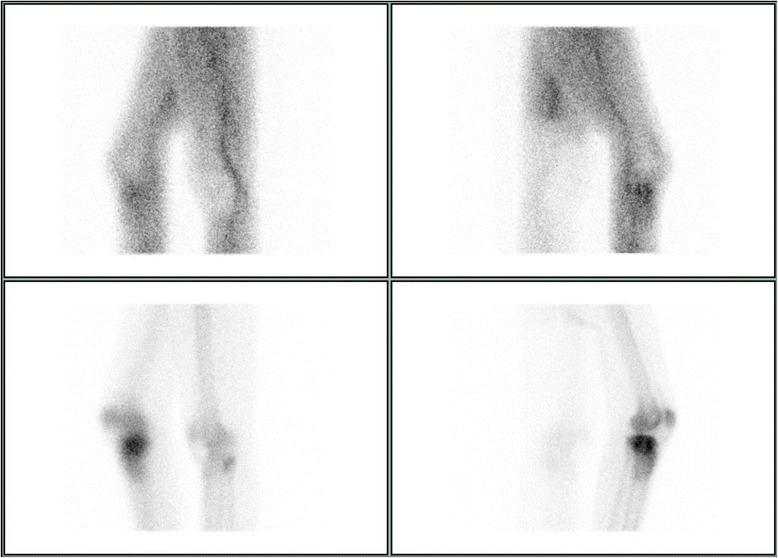
Methods: This case series evaluated available consecutive patients, whose tibial plateau fractures were treated with balloon-assisted, cement-augmented tibioplasty and received a SPECT/CT. Primary outcome variables were osseous vitality on SPECT/CTs according to the semiquantitative tracer activity analysis. The mean uptake of eight tibial regions of interest was referenced to the mean uptake count on the same region of the contralateral leg to obtain a count ratio. Osteonecrosis was defined as a photopenic area or cold defect. Secondary variables included clinical and radiological follow-up data. Statistics were carried out in a descriptive pattern.
Results: Ten patients with a mean age of 59 years and a mean follow up of 18 months were included. Calcium phosphate (CaP) substitute bone cement was used in 60% and polymethyl methacrylate mixed with hydroxyapatite (PMMA/HA) bone cement in 40%. Normal to high SPECT/CT activity without photopenic areas were observed in all patients and the mean tracer activity ratio was four, indicating vital bone in all patients. There were no postoperative infections and only one 57 year old patient with hemineglect and CaP cement showed failed osseous consolidation. The mean Tegner and Lysholm as well as the Lysholm scores were three and 80, respectively.
Conclusions: This novel study about cement-augmented balloon tibioplasties showed that osseous vitality remains intact according to SPECT/CT analysis; irrespective of the type of cement and even in the presence of thin bone lamellae. This procedure was safe and well-suited for lateral tibial plateau fractures in particular. Surgeons may consider using PMMA/HA bone cement for void filling in elderly fracture patients without concern about bone viability.
Figures







References
-
- Jacofsky D, Haidukerwych G, Scott W. Tibia plateau fractures. Philadelphia, PA, USA: Churchill Livingstone; 2006.
-
- Jöckel JA, Erhardt J, Vincenti M, Reissig J, Hoffmann R, Husain B, et al. Minimally invasive and open surgical treatment of proximal tibia fractures using a polyaxial locking plate system: a prospective multi-centre study. Int Orthop. 2013;37(4):701–8. doi: 10.1007/s00264-013-1820-x. - DOI - PMC - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
Miscellaneous
