

Observational, longitudinal study of delirium in consecutive unselected acute medical admissions: age-specific rates and associated factors, mortality and re-admission
- PMID: 26576806
- PMCID: PMC4654280
- DOI: 10.1136/bmjopen-2015-007808
Observational, longitudinal study of delirium in consecutive unselected acute medical admissions: age-specific rates and associated factors, mortality and re-admission
Abstract
Objectives: We aimed to determine age-specific rates of delirium and associated factors in acute medicine, and the impact of delirium on mortality and re-admission on long-term follow-up.
Design: Observational study. Consecutive patients over two 8-week periods (2010, 2012) were screened for delirium on admission, using the confusion assessment method (CAM), and reviewed daily thereafter. Delirium diagnosis was made using the Diagnostic and Statistical Manual Fourth Edition (DSM IV) criteria. For patients aged ≥65 years, potentially important covariables identified in previous studies were collected with follow-up for death and re-admission until January 2014.
Participants: 503 consecutive patients (age median=72, range 16-99 years, 236 (48%) male).
Setting: Acute general medicine.
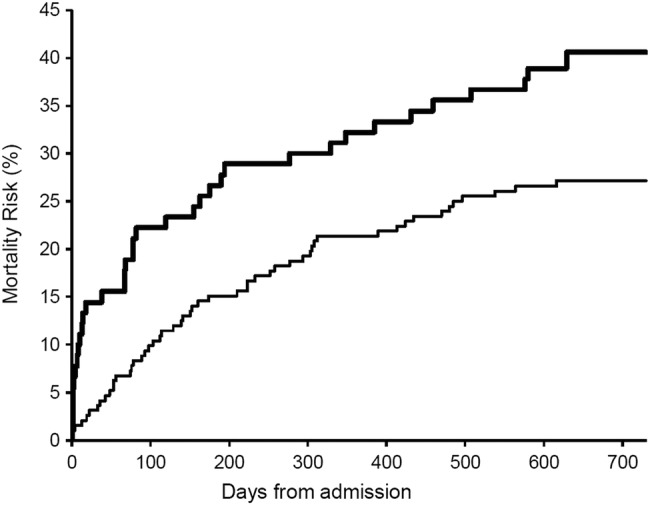
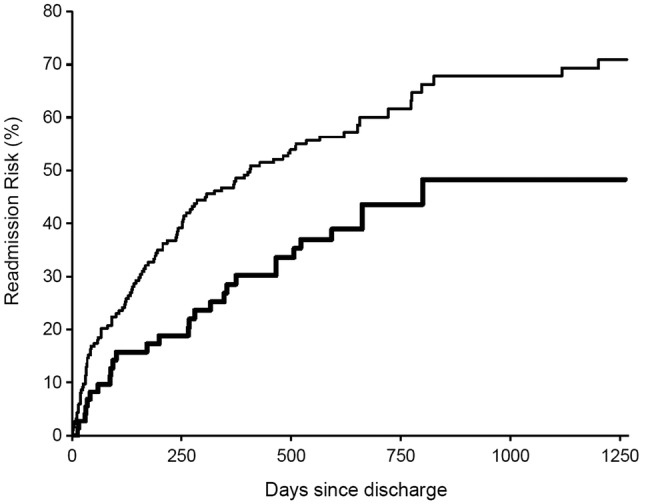
Results: Delirium occurred in 101/503 (20%) (71 on admission, 30 during admission, 17 both), with risk increasing from 3% (6/195) at <65 years to 14% (10/74) for 65-74 years and 36% (85/234) at ≥75 years (p<0.0001). Among 308 patients aged >65 years, after adjustment for age, delirium was associated with previous falls (OR=2.47, 95% CI 1.45 to 4.22, p=0.001), prior dementia (2.08, 1.10 to 3.93, p=0.024), dependency (2.58, 1.48 to 4.48, p=0.001), low cognitive score (5.00, 2.50 to 9.99, p<0.0001), dehydration (3.53, 1.91 to 6.53, p<0.0001), severe illness (1.98, 1.17 to 3.38, p=0.011), pressure sore risk (5.56, 2.60 to 11.88, p<0.0001) and infection (4.88, 2.85 to 8.36, p<0.0001). Patients with delirium were more likely to fall (OR=4.55, 1.47 to 14.05, p=0.008), be incontinent of urine (3.76, 2.15 to 6.58, p<0.0001) or faeces (3.49, 1.81-6.73, p=0.0002) and be catheterised (5.08, 2.44 to 10.54, p<0.0001); and delirium was associated with stay >7 days (2.82, 1.68 to 4.75, p<0.0001), death (4.56, 1.71 to 12.17, p=0.003) and an increase in dependency among survivors (2.56, 1.37 to 4.76, p=0.003) with excess mortality still evident at 2-year follow-up. Patients with delirium had fewer re-admissions within 30-days (OR=0.32, 95% CI 0.09 to 1.1, p=0.07) and in total (median, IQR total re-admissions=0, 0-1 vs 1, 0-2, p=0.01).
Conclusions: Delirium affected a fifth of acute medical admissions and a third of those aged ≥75 years, and was associated with increased mortality, institutionalisation and dependency, but not with increased risk of re-admission on follow-up.
Keywords: Delirium; INTERNAL MEDICINE; Mortality; Outcome; Readmission.
Published by the BMJ Publishing Group Limited. For permission to use (where not already granted under a licence) please go to http://www.bmj.com/company/products-services/rights-and-licensing/
Figures

References
-
- Delirium, diagnosis, prevention and management. National Institute for Health and Clinical Excellence (NICE) Guideline CG 103. http://www.nice.org.uk/CG103.
-
- Hospitals on the Edge, a Time for Action. Royal College Physicians, London, September, 2012. http://www.rcplondon.ac.uk/futurehospital
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical