

A cost-effectiveness analysis of three components of a syndromic surveillance system for the early warning of epidemics in rural China
- PMID: 26577518
- PMCID: PMC4650097
- DOI: 10.1186/s12889-015-2475-x
A cost-effectiveness analysis of three components of a syndromic surveillance system for the early warning of epidemics in rural China
Abstract
Background: Syndromic surveillance systems (SSSs) collect non-specific syndromes in early stages of disease outbreaks. This makes an SSS a promising tool for the early detection of epidemics. An Integrated Surveillance System in rural China (ISSC project), which added an SSS to the existing Chinese surveillance system for the early warning of epidemics, was implemented from April 2012 to March 2014 in Jiangxi and Hubei Provinces. This study aims to measure the costs and effectiveness of the three components of the SSS in the ISSC project.
Methods: The central measures of the cost-effectiveness analysis of the three components of the syndromic surveillance system were: 1) the costs per reported event, respectively, at the health facilities, the primary schools and the pharmacies; and 2) the operating costs per surveillance unit per year, respectively, at the health facilities, the primary schools and the pharmacies. Effectiveness was expressed by reporting outputs which were numbers of reported events, numbers of raw signals, and numbers of verified signals. The reported events were tracked through an internal data base. Signal verification forms and epidemiological investigation reports were collected from local country centers for disease control and prevention. We adopted project managers' perspective for the cost analysis. Total costs included set-up costs (system development and training) and operating costs (data collection, quality control and signal verification). We used self-designed questionnaires to collect cost data and received, respectively, 369 and 477 facility and staff questionnaires through a cross-sectional survey with a purposive sampling following the ISSC project. All data were entered into Epidata 3.02 and exported to Stata for descriptive analysis.
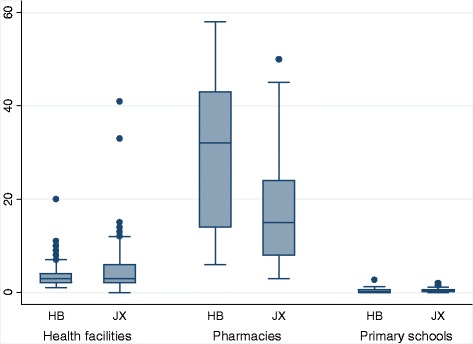
Results: The number of daily reported events per unit was the highest at pharmacies, followed by health facilities and finally primary schools. Variances existed within the three groups and also between Jiangxi and Hubei. During a 15-month surveillance period, the number of raw signals for early warning in Jiangxi province (n = 36) was nine times of that in Hubei. Health facilities and primary schools had equal numbers of raw signals (n = 19), which was 9.5 times of that from pharmacies. Five signals were confirmed as outbreaks, of which two were influenza, two were chicken pox and one was mumps. The cost per reported event was the highest at primary schools, followed by health facilities and then pharmacies. The annual operating cost per surveillance unit was the highest at pharmacies, followed by health facilities and finally primary schools. Both the cost per reported event and the annual operating cost per surveillance unit in Jiangxi in each of the three groups were higher than their counterparts in Hubei.
Conclusions: Health facilities and primary schools are better sources of syndromic surveillance data in the early warning of outbreaks. The annual operating costs of all the three components of the syndromic surveillance system in the ISSC Project were low compared to general government expenditures on health and average individual income in rural China.
Figures
Similar articles
-
Measuring costs of data collection at village clinics by village doctors for a syndromic surveillance system-a cross sectional survey from China.BMC Health Serv Res. 2015 Jul 25;15:287. doi: 10.1186/s12913-015-0965-2. BMC Health Serv Res. 2015. PMID: 26208506 Free PMC article.
-
Estimating the effectiveness of early control measures through school absenteeism surveillance in observed outbreaks at rural schools in Hubei, China.PLoS One. 2014 Sep 24;9(9):e106856. doi: 10.1371/journal.pone.0106856. eCollection 2014. PLoS One. 2014. PMID: 25250786 Free PMC article.
-
ISS--an electronic syndromic surveillance system for infectious disease in rural China.PLoS One. 2013 Apr 23;8(4):e62749. doi: 10.1371/journal.pone.0062749. Print 2013. PLoS One. 2013. PMID: 23626853 Free PMC article.
-
A Systematic Review of Methodological Variation in Healthcare Provider Perspective Tuberculosis Costing Papers Conducted in Low- and Middle-Income Settings, Using An Intervention-Standardised Unit Cost Typology.Pharmacoeconomics. 2020 Aug;38(8):819-837. doi: 10.1007/s40273-020-00910-w. Pharmacoeconomics. 2020. PMID: 32363543 Free PMC article.
-
Cost analysis of an integrated vaccine-preventable disease surveillance system in Costa Rica.Vaccine. 2013 Jul 2;31 Suppl 3(0 3):C88-93. doi: 10.1016/j.vaccine.2013.05.036. Vaccine. 2013. PMID: 23777698 Free PMC article. Review.
Cited by
-
A Practitioner-Driven Research Agenda for Syndromic Surveillance.Public Health Rep. 2017 Jul/Aug;132(1_suppl):116S-126S. doi: 10.1177/0033354917709784. Public Health Rep. 2017. PMID: 28692395 Free PMC article.
-
Spatial and Temporal Patterns of Typhoid and Paratyphoid Fever Outbreaks: A Worldwide Review, 1990-2018.Clin Infect Dis. 2019 Oct 30;69(Suppl 6):S499-S509. doi: 10.1093/cid/ciz705. Clin Infect Dis. 2019. PMID: 31665782 Free PMC article. Review.
-
Multisectoral cost analysis of a human and livestock anthrax outbreak in Songwe Region, Tanzania (December 2018-January 2019), using a novel Outbreak Costing Tool.One Health. 2021 Apr 30;13:100259. doi: 10.1016/j.onehlt.2021.100259. eCollection 2021 Dec. One Health. 2021. PMID: 34013015 Free PMC article.
References
-
- World Health Organization: World Health Organization Country Cooperation Strategy at a glance-China 2014. Available at: http://www.who.int/countryfocus/cooperation_strategy/briefs2006/en/. [Accessed 2015 02 03].
-
- Huang W, Gong X. Analysis on the current situations of human resource of health care in the country of china. Yi Xue Yu She Hui. 2007;20(9):21–25.
-
- World Health Organization, Public Health and Environment, Water, Sanitation, Hygiene and Health . Scaling up household water treatment among low-income populations. 2009.
-
- Chinese CDC . The China information system for disease control and prevention. 2007.
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Miscellaneous
