

Concomitant surgical ablation for atrial fibrillation (AF) in patients with significant atrial dilation >55 mm. Worth the effort?
- PMID: 26577821
- PMCID: PMC4650117
- DOI: 10.1186/s13019-015-0337-3
Concomitant surgical ablation for atrial fibrillation (AF) in patients with significant atrial dilation >55 mm. Worth the effort?
Abstract
Background: Concomitant Surgical AF ablation is an established procedure, recommended in guidelines. However many surgeons are reluctant to perform AF ablation in patients with significantly enlarged left atrium. We therefore analyzed outcomes of patients with left-atrial diameter >55 mm undergoing concomitant AF ablation.
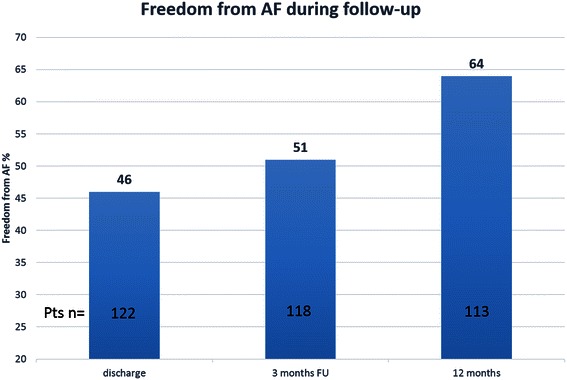
Methods: Between 05/2003 and 12/2012 124 patients with significantly enlarged left-atrium >55 mm underwent concomitant surgical AF ablation. Rhythm monitoring was accomplished by implantable loop recorder (ILR) interrogation (n = 54), or 24-h Holter-ECG (n = 70). Successful ablation was defined as AF Burden <0.5 % in ILR interrogation or absence of AF episode >30 s in 24-h Holter-ECG. Primary endpoint of the study was freedom from AF at 12 months follow-up.
Results: Mean patient's age was 65.7+/-9.6 years, 69.4 % were male. No major ablation or ILR related complications occurred. Mean LA diameter was 60.7+/-4.4 mm. Survival rate at one-year follow up was 94.4 %. 11 (8.8 %) patients received additional catheter-based ablation, while 23 (18.5 %) had an electrical cardioversion during follow-up period. Overall freedom from AF rate after one-year follow-up was 64.4 % and 59.4 % off antiarrhythmic drugs respectively. Logistic regression analysis identified preoperative paroxysmal AF, duration of AF and LA diameter > 70 mm as predictors for rhythm outcome at 12 months follow-up.
Conclusion: In this patient cohort with significantly enlarged LA diameter, concomitant surgical AF ablation provided freedom from AF of 64.4 % after one-year follow-up. However in this patient population, an accurate postoperative care with interventions like medical or- electrical cardioversion and additional catheter based ablation is necessary to achieve satisfactory results.
References
-
- Flaker GC, Belew K, Beckman K, Vidaillet H, Kron J, Safford R, et al. Asymptomatic atrial fibrillation: demographic features and prognostic information from the Atrial Fibrillation Follow-up Investigation of Rhythm Management (AFFIRM) study. Am Heart J. 2005;149:657–63. doi: 10.1016/j.ahj.2004.06.032. - DOI - PubMed
-
- Fuster V, Ryden LE, Cannom DS, Crijns HJ, Curtis AB, Ellenbogen KA, et al. 2011 ACCF/AHA/HRS focused updates incorporated into the ACC/AHA/ESC 2006 guidelines for the management of patients with atrial fibrillation: a report of the American College of Cardiology Foundation/American Heart Association Task Force on practice guidelines. Circulation. 2011;123:e269–367. doi: 10.1161/CIR.0b013e318214876d. - DOI - PubMed
-
- Calkins H, Kuck KH, Cappato R, Brugada J, Camm AJ, Chen SA, et al. 2012 HRS/EHRA/ECAS expert consensus statement on catheter and surgical ablation of atrial fibrillation: recommendations for patient selection, procedural techniques, patient management and follow-up, definitions, endpoints, and research trial design: a report of the Heart Rhythm Society (HRS) Task Force on Catheter and Surgical Ablation of Atrial Fibrillation. Developed in partnership with the European Heart Rhythm Association (EHRA), a registered branch of the European Society of Cardiology (ESC) and the European Cardiac Arrhythmia Society (ECAS); and in collaboration with the American College of Cardiology (ACC), American Heart Association (AHA), the Asia Pacific Heart Rhythm Society (APHRS), and the Society of Thoracic Surgeons (STS). Endorsed by the governing bodies of the American College of Cardiology Foundation, the American Heart Association, the European Cardiac Arrhythmia Society, the European Heart Rhythm Association, the Society of Thoracic Surgeons, the Asia Pacific Heart Rhythm Society, and the Heart Rhythm Society. Heart Rhythm. 2012;9:632–96. doi: 10.1016/j.hrthm.2011.12.016. - DOI - PubMed
-
- Cox JL, Schuessler RB, D'Agostino HJ, Jr, Stone CM, Chang BC, Cain ME, et al. The surgical treatment of atrial fibrillation. III. Development of a definitive surgical procedure. J Thorac Cardiovasc Surg. 1991;101:569–83. - PubMed
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
