

Sarcopenia in COPD: relationship with COPD severity and prognosis
- PMID: 26578132
- PMCID: PMC4635087
- DOI: 10.1590/S1806-37132015000000040
Sarcopenia in COPD: relationship with COPD severity and prognosis
Abstract
Objective: To evaluate the prevalence of sarcopenia in COPD patients, as well as to determine whether sarcopenia correlates with the severity and prognosis of COPD.
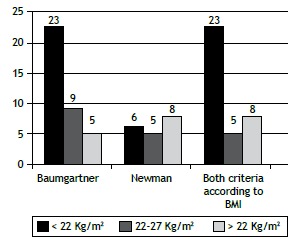
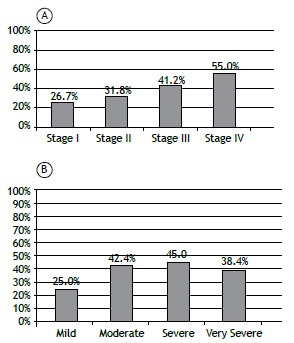
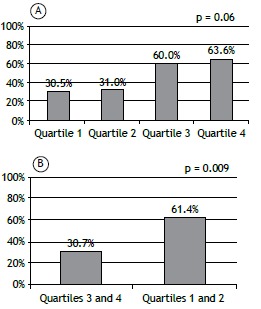
Methods: A cross-sectional study with COPD patients followed at the pulmonary outpatient clinic of our institution. The patients underwent dual-energy X-ray absorptiometry. The diagnosis of sarcopenia was made on the basis of the skeletal muscle index, defined as appendicular lean mass/height2 only for low-weight subjects and adjusted for fat mass in normal/overweight subjects. Disease severity (COPD stage) was evaluated with the Global Initiative for Chronic Obstructive Lung Disease (GOLD) criteria. The degree of obstruction and prognosis were determined by the Body mass index, airflow Obstruction, Dyspnea, and Exercise capacity (BODE) index.
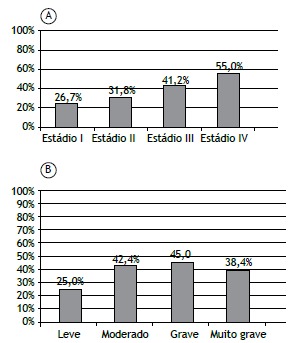
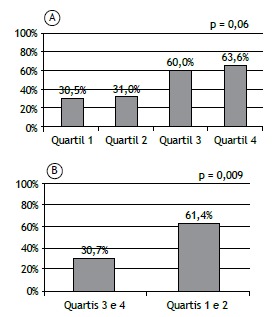
Results: We recruited 91 patients (50 females), with a mean age of 67.4 ± 8.7 years and a mean BMI of 25.8 ± 6.1 kg/m2. Sarcopenia was observed in 36 (39.6%) of the patients, with no differences related to gender, age, or smoking status. Sarcopenia was not associated with the GOLD stage or with FEV1 (used as an indicator of the degree of obstruction). The BMI, percentage of body fat, and total lean mass were lower in the patients with sarcopenia than in those without (p < 0.001). Sarcopenia was more prevalent among the patients in BODE quartile 3 or 4 than among those in BODE quartile 1 or 2 (p = 0.009). The multivariate analysis showed that the BODE quartile was significantly associated with sarcopenia, regardless of age, gender, smoking status, and GOLD stage.
Conclusions: In COPD patients, sarcopenia appears to be associated with unfavorable changes in body composition and with a poor prognosis.
Objetivo:: Avaliar a prevalência de sarcopenia em pacientes com DPOC e determinar se sarcopenia está correlacionada com a gravidade e o prognóstico de DPOC.
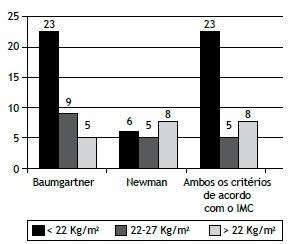
Métodos:: Estudo retrospectivo em pacientes com DPOC atendidos no ambulatório de pneumologia de nossa instituição. Os pacientes realizaram absorciometria de dupla energia por raios X. O diagnóstico de sarcopenia foi baseado no índice de massa muscular esquelética, definido como massa magra apendicular/altura2 somente para indivíduos com baixo peso, sendo ajustado pela massa gorda para aqueles com peso normal/sobrepeso. A gravidade da doença (estádio da DPOC) foi avaliada com os critérios da Global Initiative for Chronic Obstructive Lung Disease (GOLD). O grau de obstrução e o prognóstico foram determinados pelo índice Body mass index, airflow Obstruction, Dyspnea, and Exercise capacity (BODE).
Resultados:: Foram incluídos 91 pacientes (50 mulheres), com média de idade de 67,4 ± 8,7 anos e média de IMC de 25,8 ± 6,1 kg/m2. Sarcopenia foi diagnosticada em 36 (39,6%) dos pacientes, sem diferenças relacionadas a sexo, idade ou status tabágico. Não houve associação de sarcopenia com estádios GOLD ou VEF1 (utilizado como indicador do grau de obstrução). O IMC, a porcentagem de gordura corporal e a massa magra total foram menores nos pacientes com sarcopenia do que naqueles sem a doença (p < 0,001). A prevalência de sarcopenia foi maior nos pacientes com BODE nos quartis 3 ou 4 que naqueles com BODE nos quartis 1 ou 2 (p = 0,009). A análise multivariada mostrou que os quartis do BODE estavam significativamente associados à sarcopenia, independentemente de idade, gênero, status tabágico e estádio GOLD.
Conclusões:: Em pacientes com DPOC, sarcopenia parece estar associada a alterações desfavoráveis na composição corporal e pior prognóstico.
Figures
References
-
- Eagan TM, Aukrust P, Ueland T, Hardie JA, Johannessen A, Mollnes TE. Body composition and plasma levels of inflammatory biomarkers in COPD. Eur Respir J. 2010;36(5):1027–1033. http://dx.doi.org/10.1183/09031936.00194209 - DOI - PubMed
-
- Maltais F. Body composition in COPD: looking beyond BMI. Int J Tuberc Lung Dis. 2014;18(1):3–4. http://dx.doi.org/10.5588/ijtld.13.0868 - DOI - PubMed
-
- Vilaró J, Ramirez-Sarmiento A, Martínez-Llorens JM, Mendoza T, Alvarez M, Sánchez-Cayado N. Global muscle dysfunction as a risk factor of readmission to hospital due to COPD exacerbations. Respir Med. 2010;104(12):1896–1902. http://dx.doi.org/10.1016/j.rmed.2010.05.001 - DOI - PubMed
-
- Schols AM, Broekhuizen R, Weling-Scheepers CA, Wouters EF. Body composition and mortality in chronic obstructive pulmonary disease. Am J Clin Nutr. 2005;82(1):53–59. http://dx.doi.org/10.1016/j.rmedu.2005.09.028 - DOI - PubMed
-
- Marquis K, Debigaré R, Lacasse Y, LeBlanc P, Jobin J, Carrier G, Maltais F. Midthigh muscle cross-sectional area is a better predictor of mortality than body mass index in patients with chronic obstructive pulmonary disease. Am J Respir Crit Care Med. 2002;166(6):809–813. http://dx.doi.org/10.1164/rccm.2107031 - DOI - PubMed
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
