

Laboratory Measures as Proxies for Primary Care Encounters: Implications for Quantifying Clinical Retention Among HIV-Infected Adults in North America
- PMID: 26578717
- PMCID: PMC4655744
- DOI: 10.1093/aje/kwv181
Laboratory Measures as Proxies for Primary Care Encounters: Implications for Quantifying Clinical Retention Among HIV-Infected Adults in North America
Abstract
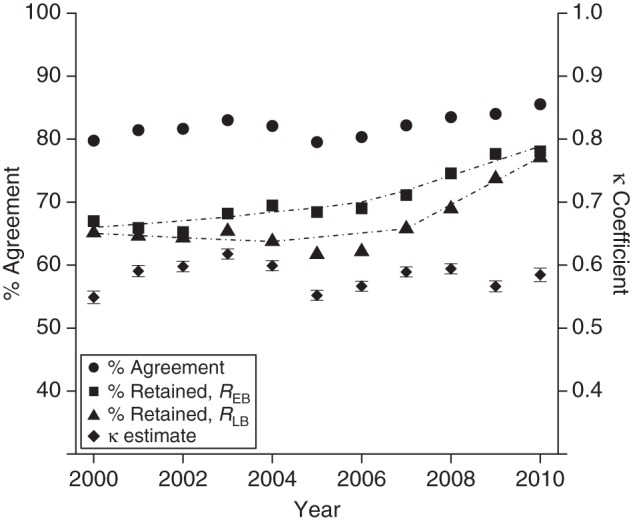
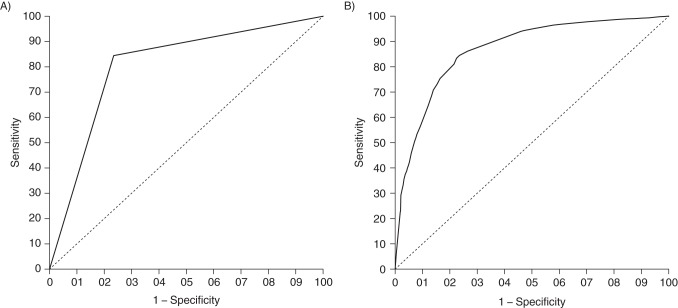
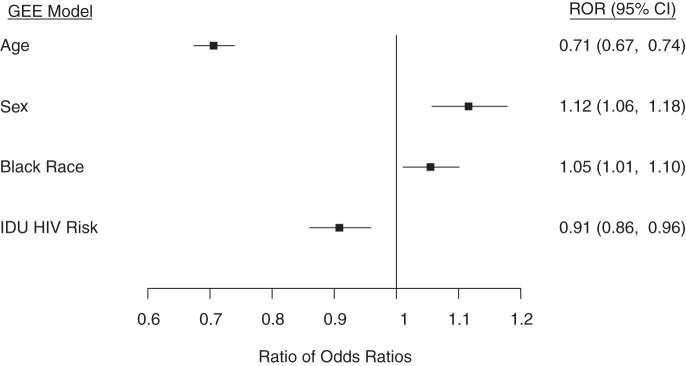
Because of limitations in the availability of data on primary care encounters, patient retention in human immunodeficiency virus (HIV) care is often estimated using laboratory measurement dates as proxies for clinical encounters, leading to possible outcome misclassification. This study included 83,041 HIV-infected adults from 14 clinical cohorts in the North American AIDS Cohort Collaboration on Research and Design (NA-ACCORD) who had ≥1 HIV primary care encounters during 2000-2010, contributing 468,816 person-years of follow-up. Encounter-based retention (REB) was defined as ≥2 encounters in a calendar year, ≥90 days apart. Laboratory-based retention (RLB) was defined similarly, using the dates of CD4-positive cell counts or HIV-1 RNA measurements. Percentage of agreement and the κ statistic were used to characterize agreement between RLB and REB. Logistic regression with generalized estimating equations and stabilized inverse-probability-of-selection weights was used to elucidate temporal trends and the discriminatory power of RLB as a predictor of REB, accounting for age, sex, race/ethnicity, primary HIV risk factor, and cohort site as potential confounders. Both REB and RLB increased from 2000 to 2010 (from 67% to 78% and from 65% to 77%, respectively), though REB was higher than RLB throughout (P < 0.01). RLB agreed well with REB (80%-86% agreement; κ = 0.55-0.62, P < 0.01) and had a strong, imperfect ability to discriminate between persons retained and not retained in care by REB (C statistic: C = 0.81, P < 0.05). As a proxy for REB, RLB had a sensitivity and specificity of 84% and 77%, respectively, with misclassification error of 18%.
Keywords: HIV; clinical encounters; clinical retention; laboratory measurements; measurement error; misclassification; proxies.
© The Author 2015. Published by Oxford University Press on behalf of the Johns Hopkins Bloomberg School of Public Health. All rights reserved. For permissions, please e-mail: journals.permissions@oup.com.
Figures
References
-
- Armenian HK, Shapiro S. Epidemiology and Health Services. New York, NY: Oxford University Press; 1998.
-
- Galea S. An argument for a consequentialist epidemiology. Am J Epidemiol. 2013;1788:1185–1191. - PubMed
-
- Cates W., Jr Invited commentary: consequential(ist) epidemiology: let's seize the day. Am J Epidemiol. 2013;1788:1192–1194. - PubMed
-
- Giordano TP, Gifford AL, White AC Jr et al. . Retention in care: a challenge to survival with HIV infection. Clin Infect Dis. 2007;4411:1493–1499. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
- K24 DA000432/DA/NIDA NIH HHS/United States
- U01 AI038855/AI/NIAID NIH HHS/United States
- K01 AI071754/AI/NIAID NIH HHS/United States
- R01 AA016893/AA/NIAAA NIH HHS/United States
- U01-AI34989/AI/NIAID NIH HHS/United States
- P30 AI027767/AI/NIAID NIH HHS/United States
- U01 AI035042/AI/NIAID NIH HHS/United States
- U01-AI38855/AI/NIAID NIH HHS/United States
- CBR-86906/CAPMC/ CIHR/Canada
- P30 MH062246/MH/NIMH NIH HHS/United States
- R01-AA16893/AA/NIAAA NIH HHS/United States
- U01 AI069434/AI/NIAID NIH HHS/United States
- R24-AI067039/AI/NIAID NIH HHS/United States
- U01 AI037984/AI/NIAID NIH HHS/United States
- U01-HD32632/HD/NICHD NIH HHS/United States
- R01 DA011602/DA/NIDA NIH HHS/United States
- K23 EY013707/EY/NEI NIH HHS/United States
- U01-AI34993/AI/NIAID NIH HHS/United States
- P30-MH62246/MH/NIMH NIH HHS/United States
- R56-AI102622/AI/NIAID NIH HHS/United States
- R01 CA165937/CA/NCI NIH HHS/United States
- U01-AI35043/AI/NIAID NIH HHS/United States
- Z01 CP010176/ImNIH/Intramural NIH HHS/United States
- K01- AI071754/AI/NIAID NIH HHS/United States
- TGF-96118/CAPMC/ CIHR/Canada
- U01 AI031834/AI/NIAID NIH HHS/United States
- HCP-97105/CAPMC/ CIHR/Canada
- P30 AI094189/AI/NIAID NIH HHS/United States
- U01-AI38858/AI/NIAID NIH HHS/United States
- U01 AI035004/AI/NIAID NIH HHS/United States
- G12 MD007583/MD/NIMHD NIH HHS/United States
- P30 AI054999/AI/NIAID NIH HHS/United States
- ZO1-CP010214/CP/NCI NIH HHS/United States
- R01-DA04334/DA/NIDA NIH HHS/United States
- U01-AI35040/AI/NIAID NIH HHS/United States
- U01-AI37984/AI/NIAID NIH HHS/United States
- U10-EY08052/EY/NEI NIH HHS/United States
- U54 MD007587/MD/NIMHD NIH HHS/United States
- R01 DA004334/DA/NIDA NIH HHS/United States
- U01-AI35004/AI/NIAID NIH HHS/United States
- U01-AI68636/AI/NIAID NIH HHS/United States
- UL1 RR024131/RR/NCRR NIH HHS/United States
- P30-AI036219/AI/NIAID NIH HHS/United States
- U01 AI034989/AI/NIAID NIH HHS/United States
- P30 AI50410/AI/NIAID NIH HHS/United States
- U01-AI68634/AI/NIAID NIH HHS/United States
- U01 AI037613/AI/NIAID NIH HHS/United States
- U01-AI69432/AI/NIAID NIH HHS/United States
- P30-AI094189/AI/NIAID NIH HHS/United States
- P30 AI045008/AI/NIAID NIH HHS/United States
- UM1 AI068634/AI/NIAID NIH HHS/United States
- U01-AI35042/AI/NIAID NIH HHS/United States
- CBR-94036/CAPMC/ CIHR/Canada
- U54-MD007587/MD/NIMHD NIH HHS/United States
- U01 AI035041/AI/NIAID NIH HHS/United States
- R24 AI067039/AI/NIAID NIH HHS/United States
- U01-AI37613/AI/NIAID NIH HHS/United States
- U01-AI069918/AI/NIAID NIH HHS/United States
- U01-AA013566/AA/NIAAA NIH HHS/United States
- U01 AI069432/AI/NIAID NIH HHS/United States
- U01-AI42590/AI/NIAID NIH HHS/United States
- U01 AI038858/AI/NIAID NIH HHS/United States
- F31 DA035713/DA/NIDA NIH HHS/United States
- MO1-RR-00052/RR/NCRR NIH HHS/United States
- R01-DA12568/DA/NIDA NIH HHS/United States
- U10 EY008057/EY/NEI NIH HHS/United States
- UL1-RR024131/RR/NCRR NIH HHS/United States
- U01 AI068636/AI/NIAID NIH HHS/United States
- U01-AI31834/AI/NIAID NIH HHS/United States
- U01 AI034994/AI/NIAID NIH HHS/United States
- U01-AI69434/AI/NIAID NIH HHS/United States
- M01 RR000052/RR/NCRR NIH HHS/United States
- K24-DA00432/DA/NIDA NIH HHS/United States
- U10 EY008052/EY/NEI NIH HHS/United States
- P30-AI27757/AI/NIAID NIH HHS/United States
- U01 AA020790/AA/NIAAA NIH HHS/United States
- P30 AI110527/AI/NIAID NIH HHS/United States
- P30 AI027763/AI/NIAID NIH HHS/United States
- K01 AI093197/AI/NIAID NIH HHS/United States
- U01 AI069918/AI/NIAID NIH HHS/United States
- U01-AA020790/AA/NIAAA NIH HHS/United States
- UL1-TR000083/TR/NCATS NIH HHS/United States
- U01-AI35041/AI/NIAID NIH HHS/United States
- U01 AA013566/AA/NIAAA NIH HHS/United States
- N02 CP055504/CP/NCI NIH HHS/United States
- U01 AI035043/AI/NIAID NIH HHS/United States
- UL1 TR000083/TR/NCATS NIH HHS/United States
- P30 AI027757/AI/NIAID NIH HHS/United States
- U01-AI35039/AI/NIAID NIH HHS/United States
- R01 DA012568/DA/NIDA NIH HHS/United States
- U10-EY08067/EY/NEI NIH HHS/United States
- P30-AI27767/AI/NIAID NIH HHS/United States
- F31-DA035713/DA/NIDA NIH HHS/United States
- U01 AI035040/AI/NIAID NIH HHS/United States
- R56 AI102622/AI/NIAID NIH HHS/United States
- K01-AI093197/AI/NIAID NIH HHS/United States
- U01 AI034993/AI/NIAID NIH HHS/United States
- R01-DA11602/DA/NIDA NIH HHS/United States
- G12-MD007583/MD/NIMHD NIH HHS/United States
- U01-AI34994/AI/NIAID NIH HHS/United States
- K23 MH097647/MH/NIMH NIH HHS/United States
- U01 AI035039/AI/NIAID NIH HHS/United States
- U24-AA020794/AA/NIAAA NIH HHS/United States
- U10-EY08057/EY/NEI NIH HHS/United States
- U10 EY008067/EY/NEI NIH HHS/United States
- P30 AI036219/AI/NIAID NIH HHS/United States
- U24 AA020794/AA/NIAAA NIH HHS/United States
- U01 AI068634/AI/NIAID NIH HHS/United States
- P30 AI050410/AI/NIAID NIH HHS/United States
- U01 AI042590/AI/NIAID NIH HHS/United States
- P30-AI54999/AI/NIAID NIH HHS/United States
- K23-MH097647/MH/NIMH NIH HHS/United States
- U01 HD032632/HD/NICHD NIH HHS/United States
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
